Service of Nephrology and Hypertension, University of Lausanne, Lausanne, Switzerland.
University College London, London, UK.
J Nephrol. 2021 Oct;34(5):1581-1590. doi: 10.1007/s40620-021-01025-x. Epub 2021 Apr 7.
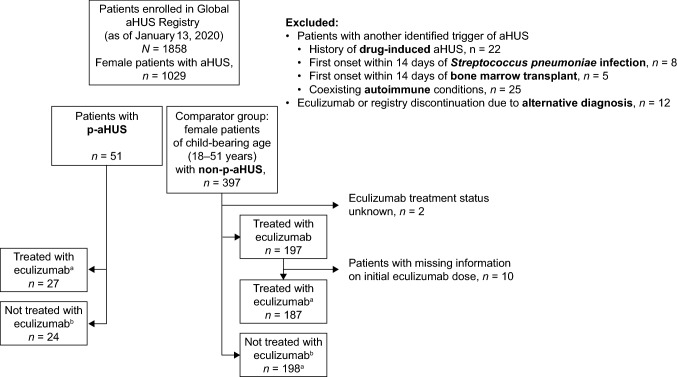
Atypical hemolytic uremic syndrome (aHUS) is a rare disease in which uncontrolled terminal complement activation leads to systemic thrombotic microangiopathy (TMA). Pregnancy can trigger aHUS and, without complement inhibition, many women with pregnancy-triggered aHUS (p-aHUS) progress to end-stage renal disease (ESRD) with a high risk of morbidity. Owing to relatively small patient numbers, published characterizations of p-aHUS have been limited, thus the Global aHUS Registry (NCT01522183, April 2012) provides a unique opportunity to analyze data from a large single cohort of women with p-aHUS.
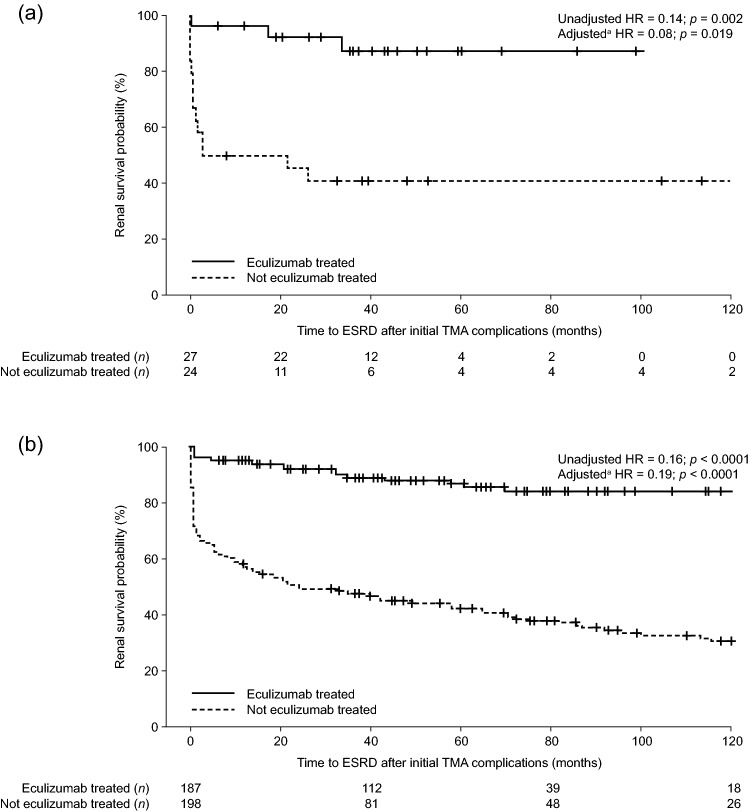
The demographics and clinical characteristics of women with p-aHUS (n = 51) were compared with those of women of childbearing age with aHUS and no identified trigger (non-p-aHUS, n = 397). Outcome evaluations, including renal survival according to time to ESRD, were compared for patients with and without eculizumab treatment (a complement C5 inhibitor) in both aHUS groups.
Baseline demographics and clinical characteristics were broadly similar in both groups. The proportion of women with p-aHUS and non-p-aHUS with pathogenic variant(s) in complement genes and/or anti-complement factor H antibodies was similar (45% and 43%, respectively), as was the proportion with a family history of aHUS (12% and 13%, respectively). Eculizumab treatment led to significantly improved renal outcomes in women with aHUS, regardless of whether aHUS was triggered by pregnancy or not: adjusted hazard ratio for time to ESRD was 0.06 (p = 0.006) in the p-aHUS group and 0.20 (p < 0.0001) in the non-p-aHUS group.
Findings from this study support the characterization of p-aHUS as a complement-mediated TMA.
非典型溶血尿毒综合征(aHUS)是一种罕见的疾病,其特征为末端补体失控激活导致全身血栓性微血管病(TMA)。妊娠可引发 aHUS,如果不抑制补体,许多妊娠诱发的 aHUS(p-aHUS)患者会进展为终末期肾病(ESRD),且发病率较高。由于患者人数相对较少,目前对 p-aHUS 的描述性研究有限,因此全球 aHUS 登记研究(NCT01522183,2012 年 4 月)为分析大量 p-aHUS 女性患者的数据提供了一个独特的机会。
比较了 51 例 p-aHUS 女性患者的人口统计学和临床特征与未发现诱因的生育年龄妇女的 aHUS 患者(非 p-aHUS,n=397)的特征。比较了两组中接受和未接受依库珠单抗(一种补体 C5 抑制剂)治疗的患者的预后评估,包括根据 ESRD 时间的肾脏生存情况。
两组患者的基线人口统计学和临床特征大致相似。p-aHUS 和非 p-aHUS 患者中补体基因和/或抗补体因子 H 抗体致病性变异的比例相似(分别为 45%和 43%),有家族性 aHUS 病史的比例也相似(分别为 12%和 13%)。无论 aHUS 是否由妊娠引发,依库珠单抗治疗均可显著改善 aHUS 患者的肾脏预后:p-aHUS 组达到 ESRD 的时间调整风险比为 0.06(p=0.006),非 p-aHUS 组为 0.20(p<0.0001)。
这项研究的结果支持将 p-aHUS 作为一种补体介导的 TMA 进行表征。