Department of Renal Medicine, Salford Royal NHS Foundation Trust, Salford, United Kingdom.
Department of Biostatistics and Medical Informatics, Acibadem Mehmet Ali Aydinlar University, Istanbul, Turkey.
PLoS One. 2019 Jul 18;14(7):e0219828. doi: 10.1371/journal.pone.0219828. eCollection 2019.
Acute kidney injury (AKI) and chronic kidney disease (CKD) are common syndromes associated with significant morbidity, mortality and cost. The extent to which repeated AKI episodes may cumulatively affect the rate of progression of all-cause CKD has not previously been investigated. In this study, we explored the hypothesis that repeated episodes of AKI increase the rate of renal functional deterioration loss in patients recruited to a large, all-cause CKD cohort.
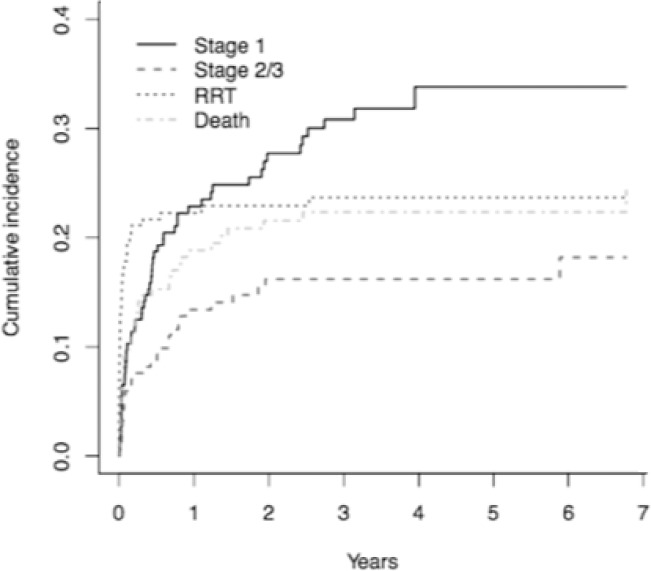
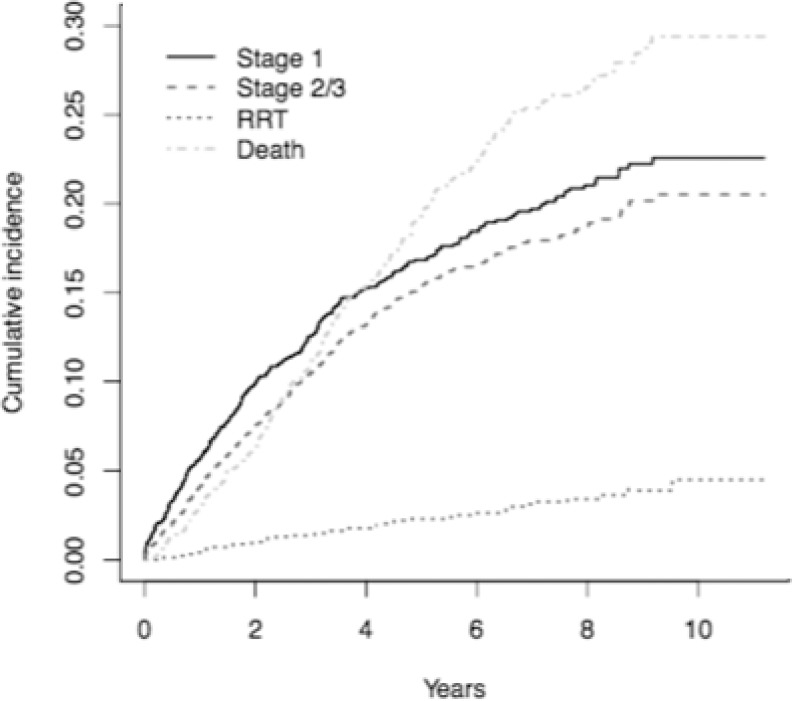
Patients from the Salford Kidney Study (SKS) were considered. Application of KDIGO criteria to all available laboratory measurements of renal function identified episodes of AKI. A competing risks model was specified for four survival events: Stage 1 AKI; stage 2 or 3 AKI; dialysis initiation or transplant before AKI event; death before AKI event. The model was adjusted for patient age, gender, smoking status, alcohol intake, diabetic status, cardiovascular co-morbidities, and primary renal disease. Analyses were performed for patients' first, second, and third or more AKI episodes.
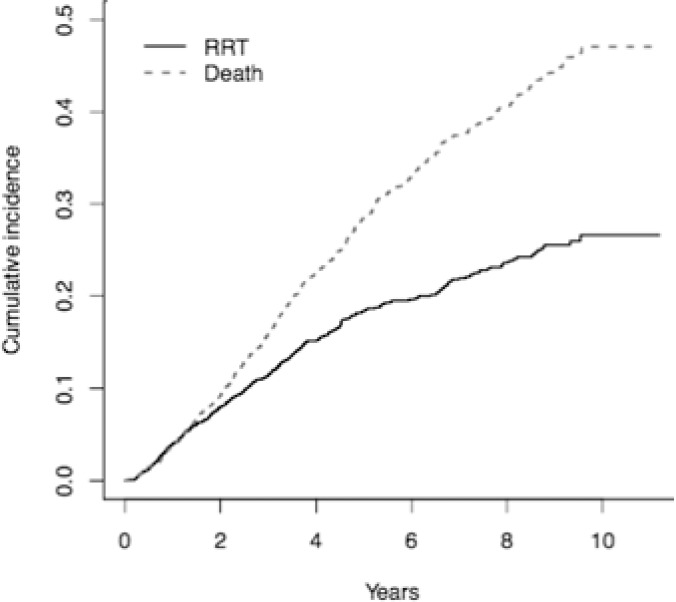
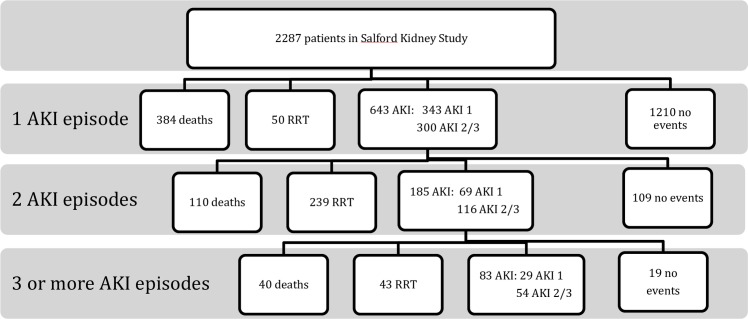
A total of 48,338 creatinine measurements were available for 2287 patients (median 13 measures per patient [IQR 6-26]). There was a median age of 66.8years, median eGFR of 28.4 and 31.6% had type 1 or 2 diabetes. Six hundred and forty three (28.1%) patients suffered one or more AKI events; 1000 AKI events (58% AKI 1) in total were observed over a median follow-up of 2.6 years [IQR 1.1-3.2]. In patients who suffered an AKI, a second AKI was more likely to be a stage 2 or 3 AKI than stage 1 [HR 2.04, p 0.01]. AKI events were associated with progression to RRT, with multiple episodes of AKI progressively increasing likelihood of progression to RRT [HR 14.4 after 1 episode of AKI, HR 28.4 after 2 episodes of AKI]. However, suffering one or more AKI events was not associated with an increased risk of mortality.
AKI events are associated with more rapid CKD deterioration as hypothesised, and also with a greater severity of subsequent AKI. However, our study did not find an association of AKI with increased mortality risk in this CKD cohort.
急性肾损伤 (AKI) 和慢性肾脏病 (CKD) 是常见的综合征,与较高的发病率、死亡率和医疗费用相关。重复发生 AKI 事件对所有 CKD 病因进展速度的累积影响程度,此前尚未被研究过。在这项研究中,我们假设重复发生 AKI 会增加进入大规模全因 CKD 队列患者的肾功能恶化(丧失)速度,并对此假说进行了探索。
研究纳入了 Salford Kidney Study (SKS) 的患者。通过对所有可用的肾功能实验室检测值应用 KDIGO 标准,识别 AKI 事件。针对四种生存事件(1 期 AKI、2 期或 3 期 AKI、AKI 事件前开始透析或移植、AKI 事件前死亡),指定了竞争风险模型。该模型调整了患者的年龄、性别、吸烟状况、饮酒状况、糖尿病状况、心血管合并症和主要肾脏疾病。对患者的首次、第二次和第三次或更多次 AKI 发作进行了分析。
共有 2287 名患者的 48338 次肌酐测量值(中位数为每位患者 13 次测量值[IQR 6-26])可用。患者的中位年龄为 66.8 岁,中位 eGFR 为 28.4%,1 型或 2 型糖尿病患者占 31.6%。643 名(28.1%)患者发生了一次或多次 AKI 事件;中位随访时间为 2.6 年(IQR 1.1-3.2)期间,共观察到 1000 次 AKI 事件(58%为 1 期 AKI)。在发生 AKI 的患者中,第二次 AKI 更可能是 2 期或 3 期 AKI,而不是 1 期 AKI(HR 2.04,p=0.01)。AKI 事件与向 RRT 进展相关,发生多次 AKI 与向 RRT 进展的可能性增加相关(发生 1 次 AKI 后 HR 为 14.4,发生 2 次 AKI 后 HR 为 28.4)。然而,发生一次或多次 AKI 事件与增加的死亡率风险无关。
正如假设的那样,AKI 事件与 CKD 恶化的速度加快有关,也与随后 AKI 的严重程度增加有关。然而,在本 CKD 队列中,我们的研究并未发现 AKI 与增加的死亡率风险之间存在关联。