Ahn Joseph C, Lauzon Marie, Luu Michael, Friedman Marc L, Kosari Kambiz, Nissen Nicholas, Lu Shelly C, Roberts Lewis R, Singal Amit G, Yang Ju Dong
Mayo Clinic, United States.
Cedars-Sinai Medical Center, United States.
J Nucl Med. 2021 Apr 9;62(12):1692-701. doi: 10.2967/jnumed.121.261954.
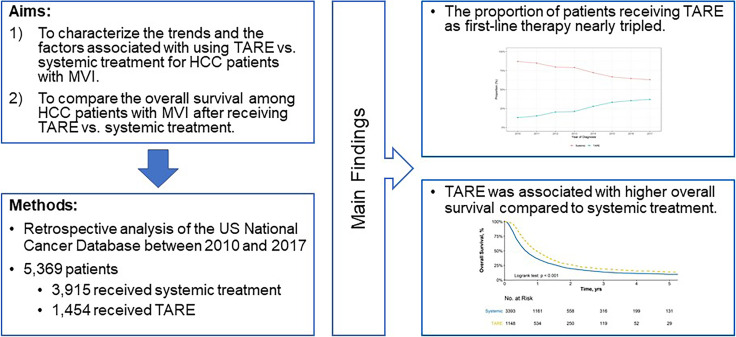
Systemic therapy remains the recommended first-line treatment for hepatocellular carcinoma (HCC) with macrovascular invasion (MVI). Transarterial radioembolization (TARE) is a promising alternative treatment given superior quality of life. The aims of this study were to 1) characterize trends and correlates for TARE as first-line treatment of HCC patients with MVI in the US and 2) compare survival after TARE versus systemic therapy. We used the US National Cancer Database to identify patients with T3BN0M0 HCC during 2010-2017. We performed multivariable logistic regression to identify factors associated with use of TARE vs. systemic therapy and Cox proportional hazards regression to identify factors associated with overall survival. Of 11,259 patients with T3BN0M0 HCC, 1454 (12.9%) and 3915 (34.7%) patients were treated with TARE and systemic therapy, respectively. The proportion of patients who received TARE increased from 13.0% in 2010 to 37.0% in 2017. Older age, White race, and receiving care at an academic cancer program were associated with receipt of TARE, while lack of insurance, higher MELD score, Charlson comorbidity Index ≥3, and Northeast region were associated with receipt of systemic therapy. TARE was associated with reduced mortality compared to systemic therapy (adjusted hazard ratio: 0.74, 95%CI: 0.68-0.80), with consistent results observed in propensity weighted analysis and across all examined subgroups. Use of TARE as first-line therapy for HCC with MVI has increased in the US. Patient characteristics, region, and medical center type affected the use of TARE. TARE was associated with reduced mortality compared to systemic therapy for HCC patients with MVI.
全身治疗仍然是伴有大血管侵犯(MVI)的肝细胞癌(HCC)推荐的一线治疗方法。鉴于其能带来更高的生活质量,经动脉放射性栓塞(TARE)是一种很有前景的替代治疗方法。本研究的目的是:1)描述美国将TARE作为伴有MVI的HCC患者一线治疗的趋势及相关因素;2)比较TARE与全身治疗后的生存率。我们使用美国国家癌症数据库来识别2010 - 2017年期间患有T3BN0M0 HCC的患者。我们进行多变量逻辑回归以识别与使用TARE vs全身治疗相关的因素,并进行Cox比例风险回归以识别与总生存相关的因素。在11259例患有T3BN0M0 HCC的患者中,分别有1454例(12.9%)和3915例(34.7%)患者接受了TARE和全身治疗。接受TARE治疗的患者比例从2010年的13.0%增加到2017年的37.0%。年龄较大、白人种族以及在学术性癌症项目机构接受治疗与接受TARE治疗相关,而缺乏保险、较高的终末期肝病模型(MELD)评分、Charlson合并症指数≥3以及东北地区与接受全身治疗相关。与全身治疗相比,TARE与死亡率降低相关(调整后的风险比:0.74,95%置信区间:0.68 - 0.80),在倾向评分加权分析以及所有检查的亚组中均观察到一致的结果。在美国,将TARE作为伴有MVI的HCC的一线治疗方法的使用有所增加。患者特征、地区和医疗中心类型影响了TARE的使用。与全身治疗相比,TARE与伴有MVI的HCC患者的死亡率降低相关。