Department of Molecular and Clinical Pharmacology, University of Liverpool, Liverpool, UK.
Department of Health Data Science, University of Liverpool, Liverpool, UK.
Lancet. 2021 Apr 10;397(10282):1363-1374. doi: 10.1016/S0140-6736(21)00247-6.
Levetiracetam and zonisamide are licensed as monotherapy for patients with focal epilepsy, but there is uncertainty as to whether they should be recommended as first-line treatments because of insufficient evidence of clinical effectiveness and cost-effectiveness. We aimed to assess the long-term clinical effectiveness and cost-effectiveness of levetiracetam and zonisamide compared with lamotrigine in people with newly diagnosed focal epilepsy.
This randomised, open-label, controlled trial compared levetiracetam and zonisamide with lamotrigine as first-line treatment for patients with newly diagnosed focal epilepsy. Adult and paediatric neurology services across the UK recruited participants aged 5 years or older (with no upper age limit) with two or more unprovoked focal seizures. Participants were randomly allocated (1:1:1) using a minimisation programme with a random element utilising factor to receive lamotrigine, levetiracetam, or zonisamide. Participants and investigators were not masked and were aware of treatment allocation. SANAD II was designed to assess non-inferiority of both levetiracetam and zonisamide to lamotrigine for the primary outcome of time to 12-month remission. Anti-seizure medications were taken orally and for participants aged 12 years or older the initial advised maintenance doses were lamotrigine 50 mg (morning) and 100 mg (evening), levetiracetam 500 mg twice per day, and zonisamide 100 mg twice per day. For children aged between 5 and 12 years the initial daily maintenance doses advised were lamotrigine 1·5 mg/kg twice per day, levetiracetam 20 mg/kg twice per day, and zonisamide 2·5 mg/kg twice per day. All participants were included in the intention-to-treat (ITT) analysis. The per-protocol (PP) analysis excluded participants with major protocol deviations and those who were subsequently diagnosed as not having epilepsy. Safety analysis included all participants who received one dose of any study drug. The non-inferiority limit was a hazard ratio (HR) of 1·329, which equates to an absolute difference of 10%. A HR greater than 1 indicated that an event was more likely on lamotrigine. The trial is registered with the ISRCTN registry, 30294119 (EudraCt number: 2012-001884-64).
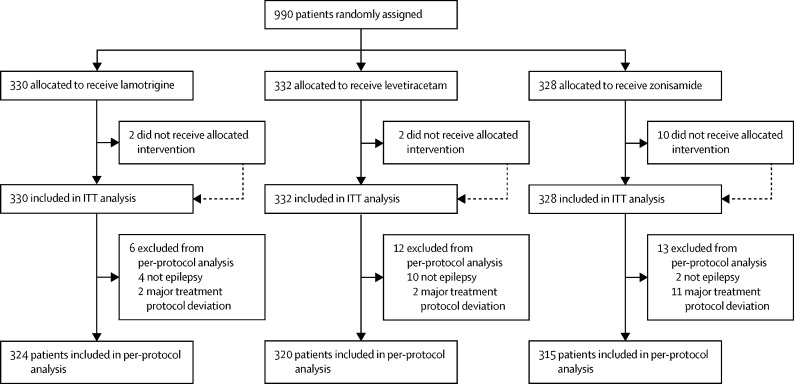
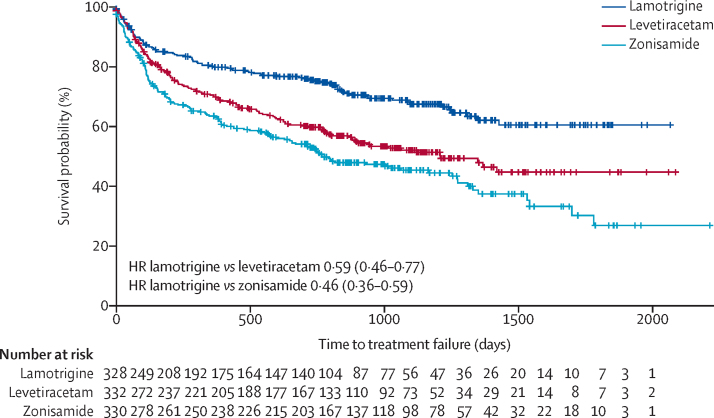
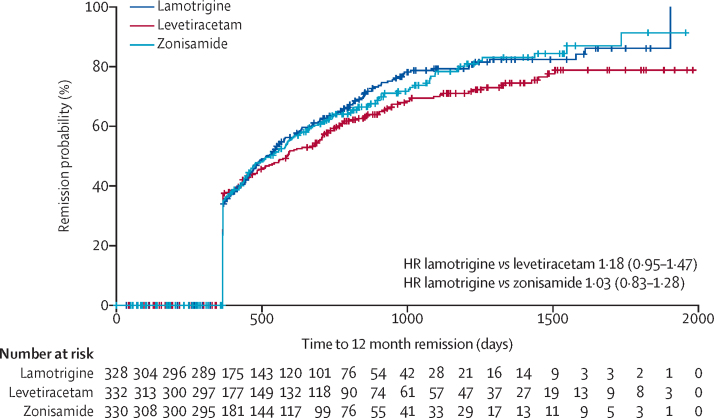
990 participants were recruited between May 2, 2013, and June 20, 2017, and followed up for a further 2 years. Patients were randomly assigned to receive lamotrigine (n=330), levetiracetam (n=332), or zonisamide (n=328). The ITT analysis included all participants and the PP analysis included 324 participants randomly assigned to lamotrigine, 320 participants randomly assigned to levetiracetam, and 315 participants randomly assigned to zonisamide. Levetiracetam did not meet the criteria for non-inferiority in the ITT analysis of time to 12-month remission versus lamotrigine (HR 1·18; 97·5% CI 0·95-1·47) but zonisamide did meet the criteria for non-inferiority in the ITT analysis versus lamotrigine (1·03; 0·83-1·28). The PP analysis showed that 12-month remission was superior with lamotrigine than both levetiracetam (HR 1·32 [97·5% CI 1·05 to 1·66]) and zonisamide (HR 1·37 [1·08-1·73]). There were 37 deaths during the trial. Adverse reactions were reported by 108 (33%) participants who started lamotrigine, 144 (44%) participants who started levetiracetam, and 146 (45%) participants who started zonisamide. Lamotrigine was superior in the cost-utility analysis, with a higher net health benefit of 1·403 QALYs (97·5% central range 1·319-1·458) compared with 1·222 (1·110-1·283) for levetiracetam and 1·232 (1·112, 1·307) for zonisamide at a cost-effectiveness threshold of £20 000 per QALY. Cost-effectiveness was based on differences between treatment groups in costs and QALYs.
These findings do not support the use of levetiracetam or zonisamide as first-line treatments for patients with focal epilepsy. Lamotrigine should remain a first-line treatment for patients with focal epilepsy and should be the standard treatment in future trials.
National Institute for Health Research Health Technology Assessment programme.
左乙拉西坦和唑尼沙胺已获准作为局灶性癫痫患者的单药治疗药物,但由于临床疗效和成本效益证据不足,对于它们是否应被推荐为一线治疗药物存在不确定性。我们旨在评估左乙拉西坦和唑尼沙胺与拉莫三嗪相比,在新诊断为局灶性癫痫的患者中的长期临床疗效和成本效益。
这是一项随机、开放标签、对照试验,比较了左乙拉西坦和唑尼沙胺与拉莫三嗪作为新诊断为局灶性癫痫患者的一线治疗药物。英国的成人和儿科神经病学服务机构招募了年龄在 5 岁及以上(无年龄上限)、有两次或两次以上未经诱发的局灶性发作的患者。参与者被随机分配(1:1:1),使用最小化方案,其中包含一个随机元素,利用因子接受拉莫三嗪、左乙拉西坦或唑尼沙胺治疗。参与者和研究者没有被蒙蔽,并且了解治疗分配。SANAD II 旨在评估左乙拉西坦和唑尼沙胺在主要结局——12 个月缓解时间方面均不劣于拉莫三嗪。抗癫痫药物口服给药,对于 12 岁及以上的参与者,初始建议的维持剂量为拉莫三嗪 50 mg(早晨)和 100 mg(晚上)、左乙拉西坦 500 mg 每日两次和唑尼沙胺 100 mg 每日两次。对于 5 至 12 岁的儿童,建议的初始每日维持剂量为拉莫三嗪 1.5 mg/kg 每日两次、左乙拉西坦 20 mg/kg 每日两次和唑尼沙胺 2.5 mg/kg 每日两次。所有参与者均纳入意向治疗(ITT)分析。符合方案(PP)分析排除了主要方案偏差的参与者和随后被诊断为非癫痫患者的参与者。安全性分析包括接受任何研究药物一剂的所有参与者。非劣效性界限为风险比(HR)1.329,相当于绝对差异 10%。HR 大于 1 表明拉莫三嗪的事件更有可能发生。该试验在 ISRCTN 注册中心注册,注册号为 30294119(EudraCt 编号:2012-001884-64)。
2013 年 5 月 2 日至 2017 年 6 月 20 日期间招募了 990 名参与者,并进一步随访了 2 年。患者被随机分配接受拉莫三嗪(n=330)、左乙拉西坦(n=332)或唑尼沙胺(n=328)治疗。ITT 分析包括所有参与者,PP 分析包括 324 名随机分配至拉莫三嗪的参与者、320 名随机分配至左乙拉西坦的参与者和 315 名随机分配至唑尼沙胺的参与者。左乙拉西坦在 ITT 分析中未达到 12 个月缓解时间与拉莫三嗪非劣效性的标准(HR 1.18;97.5%CI 0.95-1.47),但唑尼沙胺在 ITT 分析中达到了与拉莫三嗪非劣效性的标准(HR 1.03;0.83-1.28)。PP 分析显示,与左乙拉西坦和唑尼沙胺相比,拉莫三嗪在 12 个月缓解率方面更优(HR 1.32[97.5%CI 1.05-1.66])和 1.37[1.08-1.73])。试验期间有 37 人死亡。108(33%)名开始使用拉莫三嗪的参与者、144(44%)名开始使用左乙拉西坦的参与者和 146(45%)名开始使用唑尼沙胺的参与者报告了不良反应。在成本-效用分析中,拉莫三嗪具有更高的净健康效益,为 1.403 QALYs(97.5%中心范围 1.319-1.458),而左乙拉西坦为 1.222(1.110-1.283),唑尼沙胺为 1.232(1.112,1.307),在成本效益阈值为 20000 英镑/QALY 时。成本-效果是基于治疗组之间的差异在成本和 QALYs 上。
这些发现不支持将左乙拉西坦或唑尼沙胺作为局灶性癫痫患者的一线治疗药物。拉莫三嗪应继续作为局灶性癫痫患者的一线治疗药物,并应成为未来试验的标准治疗方法。
英国国家卫生研究院卫生技术评估计划。