Department of Molecular and Clinical Pharmacology, University of Liverpool, Liverpool, UK.
Department of Health Data Science, University of Liverpool, Liverpool, UK.
Lancet. 2021 Apr 10;397(10282):1375-1386. doi: 10.1016/S0140-6736(21)00246-4.
Valproate is a first-line treatment for patients with newly diagnosed idiopathic generalised or difficult to classify epilepsy, but not for women of child-bearing potential because of teratogenicity. Levetiracetam is increasingly prescribed for these patient populations despite scarcity of evidence of clinical effectiveness or cost-effectiveness. We aimed to compare the long-term clinical effectiveness and cost-effectiveness of levetiracetam compared with valproate in participants with newly diagnosed generalised or unclassifiable epilepsy.
We did an open-label, randomised controlled trial to compare levetiracetam with valproate as first-line treatment for patients with generalised or unclassified epilepsy. Adult and paediatric neurology services (69 centres overall) across the UK recruited participants aged 5 years or older (with no upper age limit) with two or more unprovoked generalised or unclassifiable seizures. Participants were randomly allocated (1:1) to receive either levetiracetam or valproate, using a minimisation programme with a random element utilising factors. Participants and investigators were aware of treatment allocation. For participants aged 12 years or older, the initial advised maintenance doses were 500 mg twice per day for levetiracetam and valproate, and for children aged 5-12 years, the initial daily maintenance doses advised were 25 mg/kg for valproate and 40 mg/kg for levetiracetam. All drugs were administered orally. SANAD II was designed to assess the non-inferiority of levetiracetam compared with valproate for the primary outcome time to 12-month remission. The non-inferiority limit was a hazard ratio (HR) of 1·314, which equates to an absolute difference of 10%. A HR greater than 1 indicated that an event was more likely on valproate. All participants were included in the intention-to-treat (ITT) analysis. Per-protocol (PP) analyses excluded participants with major protocol deviations and those who were subsequently diagnosed as not having epilepsy. Safety analyses included all participants who received one dose of any study drug. This trial is registered with the ISRCTN registry, 30294119 (EudraCt number: 2012-001884-64).
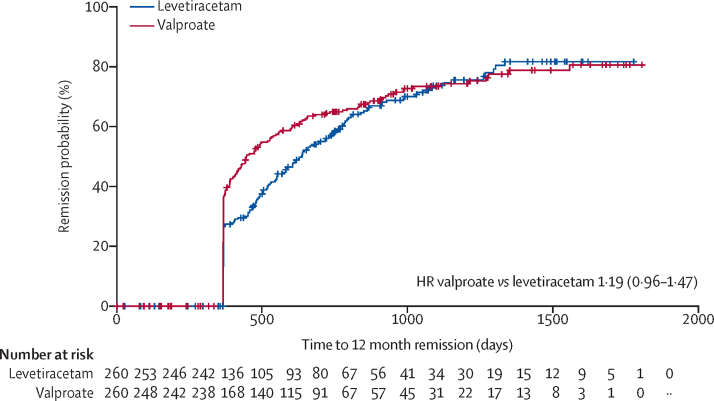
520 participants were recruited between April 30, 2013, and Aug 2, 2016, and followed up for a further 2 years. 260 participants were randomly allocated to receive levetiracetam and 260 participants to receive valproate. The ITT analysis included all participants and the PP analysis included 255 participants randomly allocated to valproate and 254 randomly allocated to levetiracetam. Median age of participants was 13·9 years (range 5·0-94·4), 65% were male and 35% were female, 397 participants had generalised epilepsy, and 123 unclassified epilepsy. Levetiracetam did not meet the criteria for non-inferiority in the ITT analysis of time to 12-month remission (HR 1·19 [95% CI 0·96-1·47]); non-inferiority margin 1·314. The PP analysis showed that the 12-month remission was superior with valproate than with levetiracetam. There were two deaths, one in each group, that were unrelated to trial treatments. Adverse reactions were reported by 96 (37%) participants randomly assigned to valproate and 107 (42%) participants randomly assigned to levetiracetam. Levetiracetam was dominated by valproate in the cost-utility analysis, with a negative incremental net health benefit of -0·040 (95% central range -0·175 to 0·037) and a probability of 0·17 of being cost-effectiveness at a threshold of £20 000 per quality-adjusted life-year. Cost-effectiveness was based on differences between treatment groups in costs and quality-adjusted life-years.
Compared with valproate, levetiracetam was found to be neither clinically effective nor cost-effective. For girls and women of child-bearing potential, these results inform discussions about benefit and harm of avoiding valproate.
National Institute for Health Research Health Technology Assessment Programme.
丙戊酸钠是新诊断的特发性全身性或难以分类的癫痫患者的一线治疗药物,但由于致畸性,不适合有生育能力的女性。左乙拉西坦越来越多地用于这些患者群体,尽管缺乏临床有效性或成本效益的证据。我们旨在比较左乙拉西坦与丙戊酸钠在新诊断的全身性或分类不明的癫痫患者中的长期临床疗效和成本效益。
我们进行了一项开放性、随机对照试验,比较左乙拉西坦与丙戊酸钠作为全身性或分类不明性癫痫患者的一线治疗药物。英国的成人和儿科神经病学服务机构(共 69 个中心)招募了年龄在 5 岁及以上(无年龄上限)、有两次或两次以上无诱因全身性或分类不明性发作的参与者。使用一种最小化方案,其中包含一个随机元素,参与者被随机分配(1:1)接受左乙拉西坦或丙戊酸钠治疗。参与者和研究人员都知道治疗分配。对于 12 岁及以上的参与者,初始建议的维持剂量为左乙拉西坦 500 mg 每日两次,丙戊酸钠 500 mg 每日两次;对于 5-12 岁的儿童,建议的初始每日维持剂量为丙戊酸钠 25 mg/kg,左乙拉西坦 40 mg/kg。所有药物均口服给药。SANAD II 旨在评估左乙拉西坦与丙戊酸钠在主要结局 12 个月缓解时间上的非劣效性。非劣效性界限为风险比(HR)为 1.314,相当于绝对差异为 10%。HR 大于 1 表明丙戊酸钠上发生事件的可能性更大。所有参与者均纳入意向治疗(ITT)分析。基于方案(PP)分析排除了有主要方案偏差的参与者和随后被诊断为无癫痫的参与者。安全性分析包括接受任何研究药物一剂的所有参与者。本试验在 ISRCTN 注册中心注册,注册号为 30294119(EudraCt 编号:2012-001884-64)。
2013 年 4 月 30 日至 2016 年 8 月 2 日期间共招募了 520 名参与者,并进行了为期 2 年的随访。260 名参与者被随机分配接受左乙拉西坦治疗,260 名参与者接受丙戊酸钠治疗。ITT 分析包括所有参与者,PP 分析包括 255 名随机分配至丙戊酸钠组和 254 名随机分配至左乙拉西坦组的参与者。参与者的中位年龄为 13.9 岁(范围为 5.0-94.4 岁),65%为男性,35%为女性,397 名参与者患有全身性癫痫,123 名患有分类不明的癫痫。左乙拉西坦在 ITT 分析中未能达到 12 个月缓解时间的非劣效性标准(HR 1.19[95%CI 0.96-1.47]);非劣效性边界为 1.314。PP 分析显示,丙戊酸钠组的 12 个月缓解率优于左乙拉西坦组。两组各有 1 例死亡,与试验治疗无关。随机分配至丙戊酸钠组的 96(37%)名参与者和随机分配至左乙拉西坦组的 107(42%)名参与者报告了不良反应。左乙拉西坦在成本效用分析中被丙戊酸钠主导,净健康效益的负增量为-0.040(95%置信区间-0.175 至 0.037),在 20000 英镑/QALY 的阈值下,具有成本效益的概率为 0.17。成本效益基于治疗组在成本和质量调整生命年方面的差异。
与丙戊酸钠相比,左乙拉西坦在临床疗效和成本效益方面均不占优势。对于女孩和有生育能力的女性,这些结果为避免使用丙戊酸钠的利弊提供了信息。
英国国家卫生与保健优化研究所卫生技术评估计划。