Froidure Antoine, Mahsouli Amin, Liistro Giuseppe, De Greef Julien, Belkhir Leila, Gérard Ludovic, Bertrand Aurélie, Koenig Sandra, Pothen Lucie, Yildiz Halil, Mwenge Benny, Aboubakar Frank, Gohy Sophie, Pilette Charles, Reychler Gregory, Coche Emmanuel, Yombi Jean-Cyr, Ghaye Benoit
Pulmonology Department, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain, Bruxelles, Belgium; Institut de Recherche Expérimentale et Clinique (IREC), Université Catholique de Louvain, Belgium.
Radiology Department, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain, Bruxelles, Belgium; Institut de Recherche Expérimentale et Clinique (IREC), Université Catholique de Louvain, Belgium.
Respir Med. 2021 May;181:106383. doi: 10.1016/j.rmed.2021.106383. Epub 2021 Apr 4.
COVID-19 pandemic resulted in an unprecedented number of hospitalizations in general wards and intensive care units (ICU). Severe and critical COVID-19 patients suffer from extensive pneumonia; therefore, long-term respiratory sequelae may be expected.
We conducted a cohort study to determine respiratory sequelae in patients with severe and critical COVID-19. We aimed at evaluating the proportion of patients with persisting respiratory symptoms and/or abnormalities in pulmonary function tests (PFT) or in lung imaging.
and methods: This is a single center cohort study including COVID-19 survivors who underwent a three-month follow-up with clinical evaluation, PFT and lung high-resolution computed tomography (HRCT). All clinical, functional, and radiological data were centrally reviewed. Multiple linear regression analysis was performed to identify factors associated with residual lesions on HRCT.
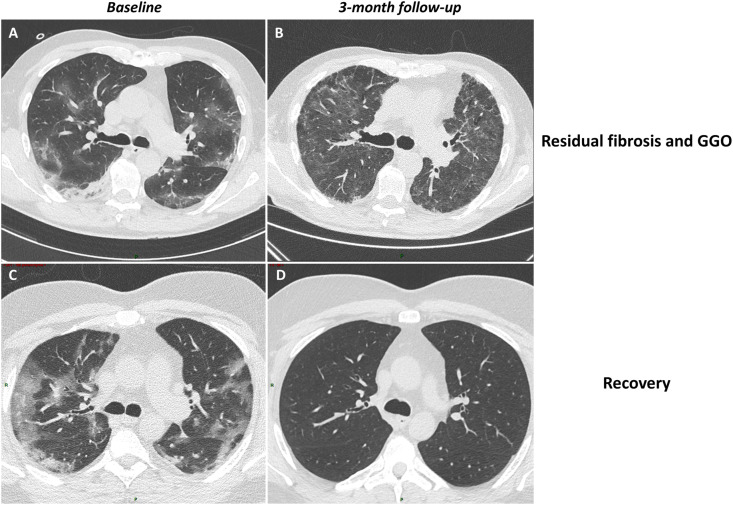
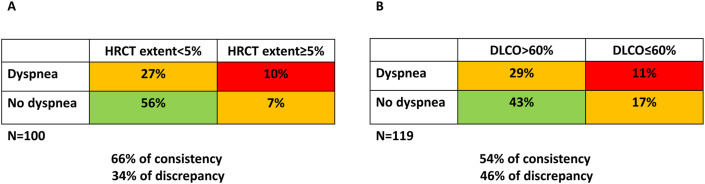
Full clinical evaluation, PFT and lung HRCT were available for central review in 126, 122 and 107 patients, respectively. At follow-up, 25% of patients complained from dyspnea and 35% from fatigue, lung diffusion capacity (DLCO) was decreased in 45%, 17% had HRCT abnormalities affecting more than 5% of their lung parenchyma while signs of fibrosis were found in 21%. In multiple linear regression model, number of days in ICU were related to the extent of persisting lesions on HRCT, while intubation was associated with signs of fibrosis at follow-up (P = 0.0005, Fisher's exact test). In contrast, the severity of lung imaging or PFT changes were not predictive of fatigue and dyspnea.
Although most hospitalized COVID-19 patients recover, a substantial proportion complains from persisting dyspnea and fatigue. Impairment of DLCO and signs suggestive of fibrosis are common but are not strictly related to long-lasting symptoms.
新冠疫情导致普通病房和重症监护病房(ICU)前所未有的住院人数。重症和危重症新冠患者患有广泛肺炎;因此,可能会出现长期呼吸后遗症。
我们进行了一项队列研究,以确定重症和危重症新冠患者的呼吸后遗症。我们旨在评估持续存在呼吸道症状和/或肺功能测试(PFT)或肺部成像异常的患者比例。
这是一项单中心队列研究,纳入了接受为期三个月随访的新冠康复者,随访内容包括临床评估、PFT和肺部高分辨率计算机断层扫描(HRCT)。所有临床、功能和放射学数据均进行集中审查。进行多元线性回归分析,以确定与HRCT残留病变相关的因素。
分别有126例、122例和107例患者的完整临床评估、PFT和肺部HRCT可供集中审查。随访时,25%的患者有呼吸困难主诉,35%有疲劳主诉,45%的患者肺弥散功能(DLCO)下降,17%的患者HRCT异常累及超过5%的肺实质,21%发现有纤维化迹象。在多元线性回归模型中,ICU住院天数与HRCT上持续病变的程度相关,而插管与随访时的纤维化迹象相关(P = 0.0005,Fisher精确检验)。相比之下,肺部成像或PFT变化的严重程度不能预测疲劳和呼吸困难。
尽管大多数住院的新冠患者康复,但相当一部分患者仍有持续的呼吸困难和疲劳主诉。DLCO受损和提示纤维化的迹象很常见,但与长期症状并无严格关联。