Nguyen Oliver T, Alishahi Tabriz Amir, Huo Jinhai, Hanna Karim, Shea Christopher M, Turner Kea
Department of Health Outcomes and Biomedical Informatics, University of Florida, Gainesville, FL, United States.
Department of Health Services Administration, University of Alabama at Birmingham, Birmingham, AL, United States.
J Med Internet Res. 2021 May 5;23(5):e27531. doi: 10.2196/27531.
Electronic visits (e-visits) involve asynchronous communication between clinicians and patients through a secure web-based platform, such as a patient portal, to elicit symptoms and determine a diagnosis and treatment plan. E-visits are now reimbursable through Medicare due to the COVID-19 pandemic. The state of evidence regarding e-visits, such as the impact on clinical outcomes and health care delivery, is unclear.
To address this gap, we examine how e-visits have impacted clinical outcomes and health care quality, access, utilization, and costs.
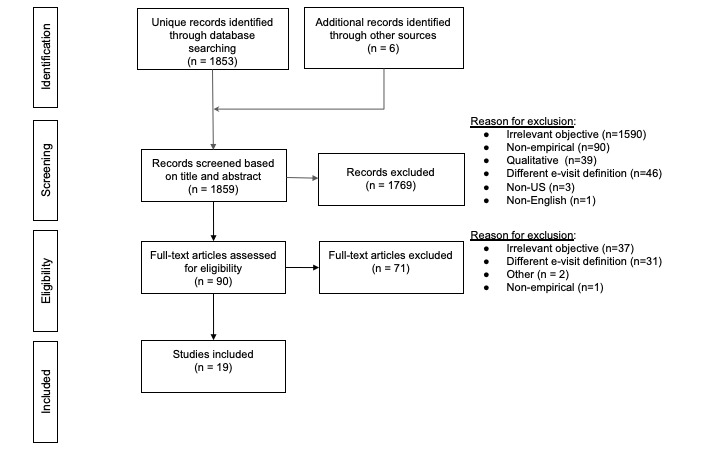
We conducted a systematic review; MEDLINE, Embase, and Web of Science were searched from January 2000 through October 2020 for peer-reviewed studies that assessed e-visits' impacts on clinical and health care delivery outcomes.
Out of 1859 papers, 19 met the inclusion criteria. E-visit usage was associated with improved or comparable clinical outcomes, especially for chronic disease management (eg, diabetes care, blood pressure management). The impact on quality of care varied across conditions. Quality of care was equivalent or better for chronic conditions, but variable quality was observed in infection management (eg, appropriate antibiotic prescribing). Similarly, the impact on health care utilization varied across conditions (eg, lower utilization for dermatology but mixed impact in primary care). Health care costs were lower for e-visits than those for in-person visits for a wide range of conditions (eg, dermatology and acute visits). No studies examined the impact of e-visits on health care access. It is difficult to draw firm conclusions about effectiveness or impact on care delivery from the studies that were included because many used observational designs.
Overall, the evidence suggests e-visits may provide clinical outcomes that are comparable to those provided by in-person care and reduce health care costs for certain health care conditions. At the same time, there is mixed evidence on health care quality, especially regarding infection management (eg, sinusitis, urinary tract infections, conjunctivitis). Further studies are needed to test implementation strategies that might improve delivery (eg, clinical decision support for antibiotic prescribing) and to assess which conditions can be managed via e-visits.
电子问诊(e-visits)涉及临床医生与患者通过安全的基于网络的平台(如患者门户网站)进行异步通信,以了解症状并确定诊断和治疗方案。由于新冠疫情,电子问诊目前可通过医疗保险获得报销。关于电子问诊的证据状况,如对临床结果和医疗服务提供的影响,尚不清楚。
为填补这一空白,我们研究了电子问诊如何影响临床结果以及医疗质量、可及性、利用率和成本。
我们进行了一项系统综述;检索了2000年1月至2020年10月期间的MEDLINE、Embase和科学引文索引,以查找评估电子问诊对临床和医疗服务提供结果影响的同行评审研究。
在1859篇论文中,19篇符合纳入标准。电子问诊的使用与改善或相当的临床结果相关,尤其是在慢性病管理方面(如糖尿病护理、血压管理)。对医疗质量的影响因病情而异。慢性病的医疗质量相当或更好,但在感染管理方面(如适当开具抗生素)观察到质量参差不齐。同样,对医疗服务利用率的影响因病情而异(如皮肤科利用率较低,但在初级保健中影响不一)。在多种病情下(如皮肤科和急性问诊),电子问诊的医疗成本低于面对面问诊。没有研究考察电子问诊对医疗服务可及性的影响。由于许多研究采用观察性设计,因此很难从纳入的研究中就电子问诊的有效性或对医疗服务提供的影响得出确凿结论。
总体而言,证据表明电子问诊可能提供与面对面护理相当的临床结果,并降低某些医疗状况的医疗成本。同时,关于医疗质量的证据不一,尤其是在感染管理方面(如鼻窦炎、尿路感染、结膜炎)。需要进一步研究来测试可能改善医疗服务提供的实施策略(如抗生素处方的临床决策支持),并评估哪些病情可以通过电子问诊进行管理。