Jonathan Geneva K, Dopke Cynthia A, Michaels Tania, Bank Andrew, Martin Clair R, Adhikari Krina, Krakauer Rachel L, Ryan Chloe, McBride Alyssa, Babington Pamela, Frauenhofer Ella, Silver Jamilah, Capra Courtney, Simon Melanie, Begale Mark, Mohr David C, Goulding Evan H
Department of Psychiatry and Behavioral Sciences, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States.
Pediatrics, Loma Linda Children's Hospital, Loma Linda, CA, United States.
JMIR Ment Health. 2021 Apr 12;8(4):e20424. doi: 10.2196/20424.
Bipolar disorder is a serious mental illness that results in significant morbidity and mortality. Pharmacotherapy is the primary treatment for bipolar disorder; however, adjunctive psychotherapy can help individuals use self-management strategies to improve outcomes. Yet access to this therapy is limited. Smartphones and other technologies have the potential to increase access to therapeutic strategies that enhance self-management while simultaneously providing real-time user feedback and provider alerts to augment care.
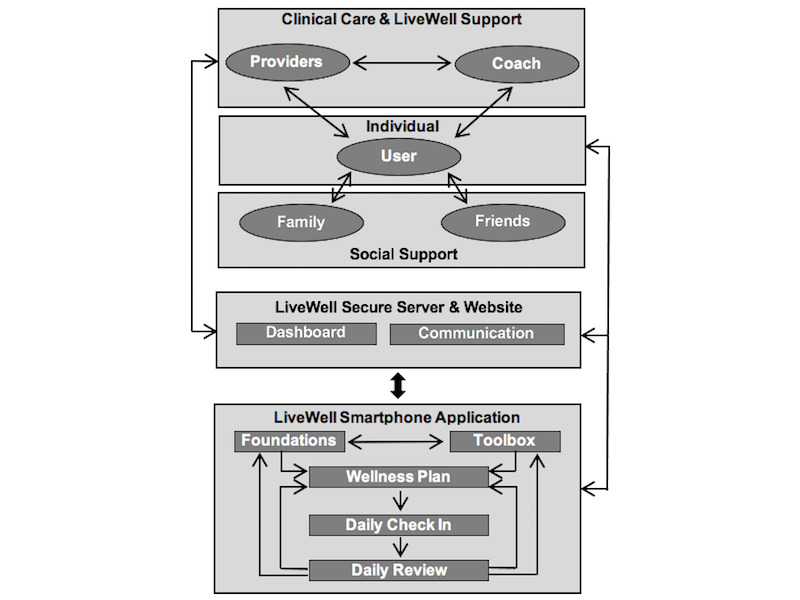
This paper describes the user-centered development of LiveWell, a smartphone-based self-management intervention for bipolar disorder, to contribute to and support the ongoing improvement and dissemination of technology-based mental health interventions.
Individuals with bipolar disorder first participated in a field trial of a simple smartphone app for self-monitoring of behavioral targets. To develop a complete technology-based intervention for bipolar disorder, this field trial was followed by design sessions, usability testing, and a pilot study of a smartphone-based self-management intervention for bipolar disorder. Throughout all phases of development, intervention revisions were made based on user feedback.
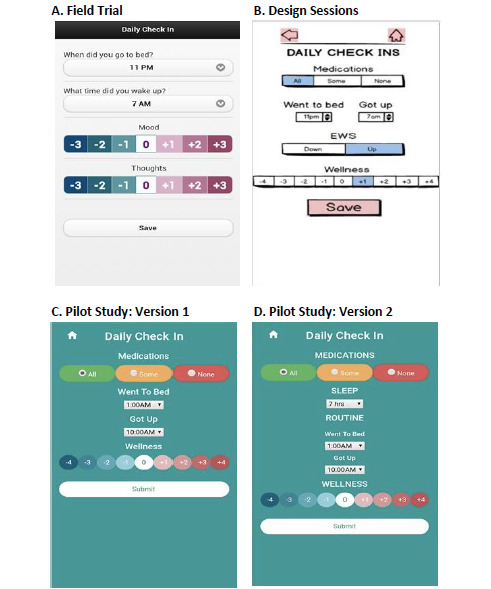
The core of the LiveWell intervention consists of a daily self-monitoring tool, the Daily Check-in. This self-monitoring tool underwent multiple revisions during the user-centered development process. Daily Check-in mood and thought rating scales were collapsed into a single wellness rating scale to accommodate user development of personalized scale anchors. These anchors are meant to assist users in identifying early warning signs and symptoms of impending episodes to take action based on personalized plans. When users identified personal anchors for the wellness scale, the anchors most commonly reflected behavioral signs and symptoms (40%), followed by cognitive (25%), mood (15%), physical (10%), and motivational (7%) signs and symptoms. Changes to the Daily Check-in were also made to help users distinguish between getting adequate sleep and keeping a regular routine. At the end of the pilot study, users reported that the Daily Check-in made them more aware of early warning signs and symptoms and how much they were sleeping. Users also reported that they liked personalizing their anchors and plans and felt this process was useful. Users experienced some difficulties with developing, tracking, and achieving target goals. Users also did not consistently follow up with app recommendations to contact providers when Daily Check-in data suggested they needed additional assistance. As a result, the human support roles for the technology were expanded beyond app use support to include support for self-management and clinical care communication. The development of these human support roles was aided by feedback on the technology's usability from the users and the coaches who provided the human support.
User input guided the development of intervention content, technology, and coaching support for LiveWell. Users valued the provision of monitoring tools and the ability to personalize plans for staying well, supporting the role of monitoring and personalization as important features of digital mental health technologies. Users also valued human support of the technology in the form of a coach, and user difficulties with aspects of self-management and care-provider communication led to an expansion of the coach's support roles. Obtaining feedback from both users and coaches played an important role in the development of both the LiveWell technology and human support. Attention to all stakeholders involved in the use of mental health technologies is essential for optimizing intervention development.
双相情感障碍是一种严重的精神疾病,会导致显著的发病率和死亡率。药物治疗是双相情感障碍的主要治疗方法;然而,辅助心理治疗可以帮助患者使用自我管理策略来改善治疗效果。然而,这种治疗方法的可及性有限。智能手机和其他技术有潜力增加获得增强自我管理的治疗策略的机会,同时提供实时用户反馈和提供者警报以加强护理。
本文描述了LiveWell的以用户为中心的开发过程,LiveWell是一款基于智能手机的双相情感障碍自我管理干预应用程序,旨在促进和支持基于技术的心理健康干预措施的持续改进和推广。
双相情感障碍患者首先参与了一个简单的智能手机应用程序的现场试验,该应用程序用于自我监测行为目标。为了开发一个完整的基于技术的双相情感障碍干预措施,在该现场试验之后进行了设计会议、可用性测试以及一项基于智能手机的双相情感障碍自我管理干预措施的试点研究。在开发的所有阶段,都根据用户反馈对干预措施进行了修订。
LiveWell干预措施的核心包括一个每日自我监测工具,即“每日签到”。在以用户为中心的开发过程中,这个自我监测工具经历了多次修订。“每日签到”的情绪和思维评分量表被合并为一个单一的健康评分量表,以适应用户制定个性化量表锚点。这些锚点旨在帮助用户识别即将发作的早期预警信号和症状,以便根据个性化计划采取行动。当用户为健康量表确定个人锚点时,这些锚点最常反映行为信号和症状(40%),其次是认知(25%)、情绪(15%)、身体(10%)和动机(7%)信号和症状。对“每日签到”也进行了修改,以帮助用户区分获得充足睡眠和保持规律作息。在试点研究结束时,用户报告说“每日签到”使他们更加意识到早期预警信号和症状以及他们的睡眠情况。用户还报告说他们喜欢个性化他们的锚点和计划,并认为这个过程很有用。用户在制定、跟踪和实现目标方面遇到了一些困难。当“每日签到”数据表明他们需要额外帮助时,用户也没有始终遵循应用程序的建议与提供者联系。因此,该技术的人力支持角色从应用程序使用支持扩展到包括自我管理和临床护理沟通支持。用户和提供人力支持的教练对技术可用性的反馈有助于这些人力支持角色的发展。
用户输入指导了LiveWell干预内容、技术和教练支持的开发。用户重视提供监测工具以及能够为保持健康制定个性化计划,这支持了监测和个性化作为数字心理健康技术重要特征的作用。用户也重视以教练形式提供的技术人力支持,并且用户在自我管理和与护理提供者沟通方面的困难导致了教练支持角色的扩展。从用户和教练那里获得反馈在LiveWell技术和人力支持的开发中都起到了重要作用。关注参与心理健康技术使用的所有利益相关者对于优化干预措施开发至关重要。