Public Health England Colindale, Colindale, London, UK; The National Institute for Health Research Health Protection Research Unit in Healthcare Associated Infections and Antimicrobial Resistance at the University of Oxford, University of Oxford, Oxford, UK.
Public Health England Colindale, Colindale, London, UK.
Lancet. 2021 Apr 17;397(10283):1459-1469. doi: 10.1016/S0140-6736(21)00675-9. Epub 2021 Apr 9.
Increased understanding of whether individuals who have recovered from COVID-19 are protected from future SARS-CoV-2 infection is an urgent requirement. We aimed to investigate whether antibodies against SARS-CoV-2 were associated with a decreased risk of symptomatic and asymptomatic reinfection.
A large, multicentre, prospective cohort study was done, with participants recruited from publicly funded hospitals in all regions of England. All health-care workers, support staff, and administrative staff working at hospitals who could remain engaged in follow-up for 12 months were eligible to join The SARS-CoV-2 Immunity and Reinfection Evaluation study. Participants were excluded if they had no PCR tests after enrolment, enrolled after Dec 31, 2020, or had insufficient PCR and antibody data for cohort assignment. Participants attended regular SARS-CoV-2 PCR and antibody testing (every 2-4 weeks) and completed questionnaires every 2 weeks on symptoms and exposures. At enrolment, participants were assigned to either the positive cohort (antibody positive, or previous positive PCR or antibody test) or negative cohort (antibody negative, no previous positive PCR or antibody test). The primary outcome was a reinfection in the positive cohort or a primary infection in the negative cohort, determined by PCR tests. Potential reinfections were clinically reviewed and classified according to case definitions (confirmed, probable, or possible) and symptom-status, depending on the hierarchy of evidence. Primary infections in the negative cohort were defined as a first positive PCR test and seroconversions were excluded when not associated with a positive PCR test. A proportional hazards frailty model using a Poisson distribution was used to estimate incidence rate ratios (IRR) to compare infection rates in the two cohorts.
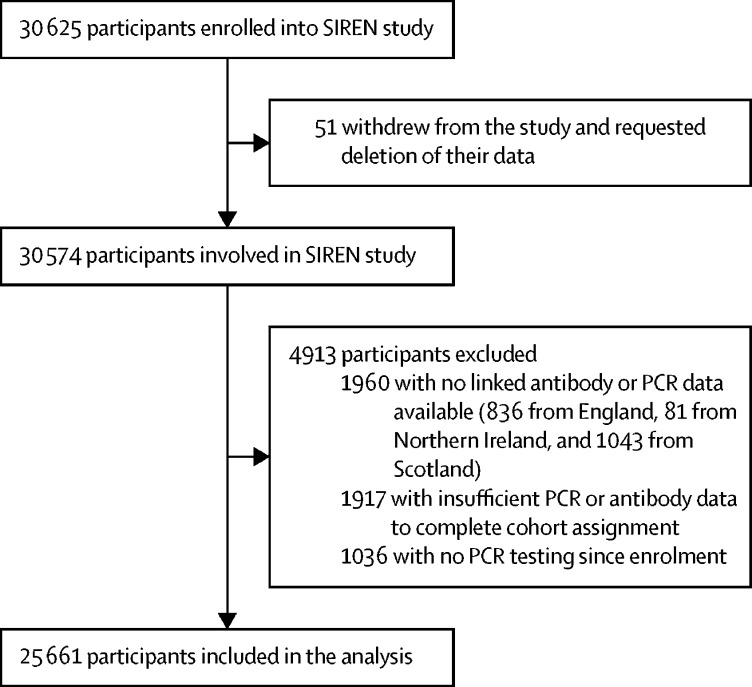
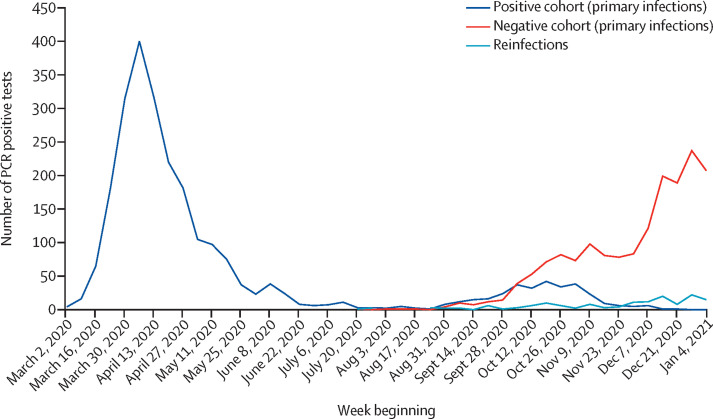
From June 18, 2020, to Dec 31, 2020, 30 625 participants were enrolled into the study. 51 participants withdrew from the study, 4913 were excluded, and 25 661 participants (with linked data on antibody and PCR testing) were included in the analysis. Data were extracted from all sources on Feb 5, 2021, and include data up to and including Jan 11, 2021. 155 infections were detected in the baseline positive cohort of 8278 participants, collectively contributing 2 047 113 person-days of follow-up. This compares with 1704 new PCR positive infections in the negative cohort of 17 383 participants, contributing 2 971 436 person-days of follow-up. The incidence density was 7·6 reinfections per 100 000 person-days in the positive cohort, compared with 57·3 primary infections per 100 000 person-days in the negative cohort, between June, 2020, and January, 2021. The adjusted IRR was 0·159 for all reinfections (95% CI 0·13-0·19) compared with PCR-confirmed primary infections. The median interval between primary infection and reinfection was more than 200 days.
A previous history of SARS-CoV-2 infection was associated with an 84% lower risk of infection, with median protective effect observed 7 months following primary infection. This time period is the minimum probable effect because seroconversions were not included. This study shows that previous infection with SARS-CoV-2 induces effective immunity to future infections in most individuals.
Department of Health and Social Care of the UK Government, Public Health England, The National Institute for Health Research, with contributions from the Scottish, Welsh and Northern Irish governments.
深入了解 COVID-19 康复者是否能免受未来 SARS-CoV-2 感染是一项紧迫的需求。我们旨在研究针对 SARS-CoV-2 的抗体是否与降低有症状和无症状再感染风险相关。
开展了一项大型的、多中心的前瞻性队列研究,参与者来自英格兰所有地区的公立医疗机构。所有能够继续参与为期 12 个月随访的医护人员、支持人员和行政人员都有资格参加 SARS-CoV-2 免疫和再感染评估研究。如果参与者在登记后没有进行 PCR 检测、在 2020 年 12 月 31 日后登记或用于队列分配的 PCR 和抗体数据不足,则将其排除在外。参与者定期接受 SARS-CoV-2 PCR 和抗体检测(每 2-4 周一次),并每两周通过问卷报告症状和接触情况。登记时,参与者被分配到阳性队列(抗体阳性,或以前的 PCR 或抗体检测阳性)或阴性队列(抗体阴性,以前没有阳性 PCR 或抗体检测)。主要结局是阳性队列的再感染或阴性队列的初次感染,通过 PCR 检测确定。根据病例定义(确诊、可能、或可能)和症状状态,对潜在再感染进行临床审查和分类,这取决于证据的层次。阴性队列中的初次感染定义为首次阳性 PCR 检测,当与阳性 PCR 检测无关时,排除血清学转换。使用泊松分布的比例风险弗拉明汉模型来估计感染率比值(IRR),以比较两个队列的感染率。
从 2020 年 6 月 18 日至 2020 年 12 月 31 日,有 30625 名参与者参加了这项研究。51 名参与者退出了研究,4913 名参与者被排除在外,25661 名参与者(具有抗体和 PCR 检测相关数据)被纳入分析。所有来源的数据均于 2021 年 2 月 5 日提取,数据截止至 2021 年 1 月 11 日。在 8278 名参与者的基线阳性队列中发现了 155 例感染,总计随访 2047113 人天。相比之下,在 17383 名参与者的 17383 名参与者的阴性队列中,有 1704 例新的 PCR 阳性感染,总计随访 2971436 人天。在 2020 年 6 月至 2021 年 1 月期间,阳性队列的感染密度为每 100000 人天 7.6 例再感染,而阴性队列的每 100000 人天 57.3 例初次感染。所有再感染的调整后 IRR 为 0.159(95%CI:0.13-0.19),与 PCR 确诊的初次感染相比。初次感染和再感染之间的中位间隔时间超过 200 天。
以前感染过 SARS-CoV-2 与感染风险降低 84%相关,在初次感染后 7 个月观察到中位数保护效果。这是因为没有包括血清学转换,所以这是最小的可能效果。这项研究表明,大多数个体以前感染过 SARS-CoV-2 会对未来的感染产生有效的免疫力。
英国政府的卫生和社会保障部、英国公共卫生部、英国国家卫生研究院,苏格兰、威尔士和北爱尔兰政府也有贡献。