Nuffield Department of Clinical Medicine, University of Oxford, Oxford, UK; National Institute for Health Research (NIHR), Oxford Biomedical Research Centre, Oxford, UK; School of Medical and Health Sciences, Edith Cowan University, Perth, WA, Australia.
Nuffield Department of Clinical Medicine, University of Oxford, Oxford, UK; UQ Centre for Clinical Research, The University of Queensland, Brisbane, QLD, Australia; School of Mathematical Sciences, Queensland University of Technology, Brisbane, QLD, Australia.
Lancet Respir Med. 2021 Jul;9(7):763-772. doi: 10.1016/S2213-2600(21)00160-0. Epub 2021 Apr 9.
Multiple early reports of patients admitted to hospital with COVID-19 showed that patients with chronic respiratory disease were significantly under-represented in these cohorts. We hypothesised that the widespread use of inhaled glucocorticoids among these patients was responsible for this finding, and tested if inhaled glucocorticoids would be an effective treatment for early COVID-19.
We performed an open-label, parallel-group, phase 2, randomised controlled trial (Steroids in COVID-19; STOIC) of inhaled budesonide, compared with usual care, in adults within 7 days of the onset of mild COVID-19 symptoms. The trial was done in the community in Oxfordshire, UK. Participants were randomly assigned to inhaled budsonide or usual care stratified for age (≤40 years or >40 years), sex (male or female), and number of comorbidities (≤1 and ≥2). Randomisation was done using random sequence generation in block randomisation in a 1:1 ratio. Budesonide dry powder was delivered using a turbohaler at a dose of 400 μg per actuation. Participants were asked to take two inhalations twice a day until symptom resolution. The primary endpoint was COVID-19-related urgent care visit, including emergency department assessment or hospitalisation, analysed for both the per-protocol and intention-to-treat (ITT) populations. The secondary outcomes were self-reported clinical recovery (symptom resolution), viral symptoms measured using the Common Cold Questionnare (CCQ) and the InFLUenza Patient Reported Outcome Questionnaire (FLUPro), body temperature, blood oxygen saturations, and SARS-CoV-2 viral load. The trial was stopped early after independent statistical review concluded that study outcome would not change with further participant enrolment. This trial is registered with ClinicalTrials.gov, NCT04416399.
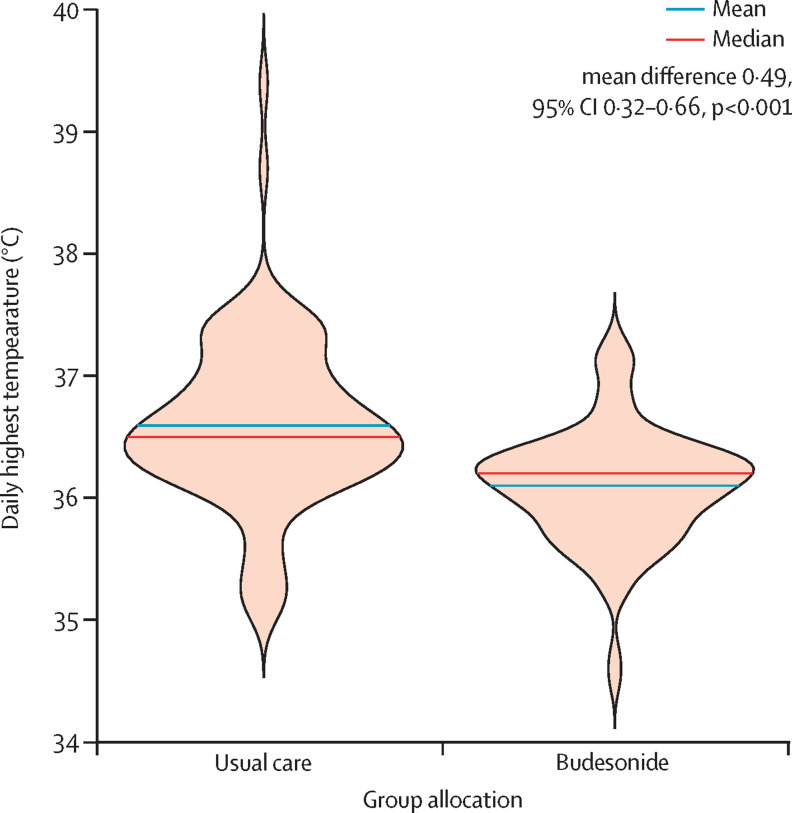
From July 16 to Dec 9, 2020, 167 participants were recruited and assessed for eligibility. 21 did not meet eligibility criteria and were excluded. 146 participants were randomly assigned-73 to usual care and 73 to budesonide. For the per-protocol population (n=139), the primary outcome occurred in ten (14%) of 70 participants in the usual care group and one (1%) of 69 participants in the budesonide group (difference in proportions 0·131, 95% CI 0·043 to 0·218; p=0·004). For the ITT population, the primary outcome occurred in 11 (15%) participants in the usual care group and two (3%) participants in the budesonide group (difference in proportions 0·123, 95% CI 0·033 to 0·213; p=0·009). The number needed to treat with inhaled budesonide to reduce COVID-19 deterioration was eight. Clinical recovery was 1 day shorter in the budesonide group compared with the usual care group (median 7 days [95% CI 6 to 9] in the budesonide group vs 8 days [7 to 11] in the usual care group; log-rank test p=0·007). The mean proportion of days with a fever in the first 14 days was lower in the budesonide group (2%, SD 6) than the usual care group (8%, SD 18; Wilcoxon test p=0·051) and the proportion of participants with at least 1 day of fever was lower in the budesonide group when compared with the usual care group. As-needed antipyretic medication was required for fewer proportion of days in the budesonide group compared with the usual care group (27% [IQR 0-50] vs 50% [15-71]; p=0·025) Fewer participants randomly assigned to budesonide had persistent symptoms at days 14 and 28 compared with participants receiving usual care (difference in proportions 0·204, 95% CI 0·075 to 0·334; p=0·003). The mean total score change in the CCQ and FLUPro over 14 days was significantly better in the budesonide group compared with the usual care group (CCQ mean difference -0·12, 95% CI -0·21 to -0·02 [p=0·016]; FLUPro mean difference -0·10, 95% CI -0·21 to -0·00 [p=0·044]). Blood oxygen saturations and SARS-CoV-2 load, measured by cycle threshold, were not different between the groups. Budesonide was safe, with only five (7%) participants reporting self-limiting adverse events.
Early administration of inhaled budesonide reduced the likelihood of needing urgent medical care and reduced time to recovery after early COVID-19.
National Institute for Health Research Biomedical Research Centre and AstraZeneca.
多项早期报告显示,患有慢性呼吸道疾病的 COVID-19 住院患者明显代表性不足。我们推测,广泛使用吸入性糖皮质激素是造成这种情况的原因,并测试吸入性糖皮质激素是否对早期 COVID-19 有效。
我们在英国牛津郡的社区中进行了一项开放性、平行组、2 期、随机对照试验(Steroids in COVID-19;STOI),比较了布地奈德吸入剂与常规护理在 COVID-19 轻症症状出现后 7 天内的疗效。试验在社区进行,参与者被随机分配接受布地奈德吸入剂或常规护理,按年龄(≤40 岁或>40 岁)、性别(男性或女性)和合并症数量(≤1 或≥2)分层。使用随机序列生成和区组随机化,以 1:1 的比例随机分组。布地奈德干粉通过涡轮吸入器给药,每次给药 400μg。参与者被要求每天吸入两次,每次两次,直到症状缓解。主要终点是 COVID-19 相关的紧急护理就诊,包括急诊评估或住院,在符合方案人群和意向治疗人群(ITT)中进行分析。次要结局是自我报告的临床康复(症状缓解)、使用普通感冒问卷(CCQ)和流感患者报告结果问卷(FLUPro)测量的病毒症状、体温、血氧饱和度和 SARS-CoV-2 病毒载量。在独立的统计审查得出研究结果不会随进一步的参与者招募而改变后,该试验提前停止。这项试验在 ClinicalTrials.gov 上注册,编号为 NCT04416399。
2020 年 7 月 16 日至 12 月 9 日,共招募了 167 名参与者进行资格评估。21 名参与者不符合入选标准,被排除在外。146 名参与者被随机分配,73 名接受常规护理,73 名接受布地奈德吸入剂治疗。对于符合方案人群(n=139),常规护理组有 10 名(14%)参与者出现主要结局,布地奈德组有 1 名(1%)参与者出现主要结局(比例差异 0.131,95%CI 0.043 至 0.218;p=0.004)。对于 ITT 人群,常规护理组有 11 名(15%)参与者出现主要结局,布地奈德组有 2 名(3%)参与者出现主要结局(差异 0.123,95%CI 0.033 至 0.213;p=0.009)。需要使用布地奈德吸入剂治疗的 COVID-19 恶化人数为 8 人。与常规护理组相比,布地奈德组的临床康复时间缩短了 1 天(布地奈德组中位数 7 天[95%CI 6 至 9],常规护理组 8 天[7 至 11];log-rank 检验 p=0.007)。在第 14 天之前,发热天数比例较低的布地奈德组(2%,SD 6),低于常规护理组(8%,SD 18;Wilcoxon 检验 p=0.051),并且与常规护理组相比,布地奈德组发热天数超过 1 天的参与者比例较低。与常规护理组相比,布地奈德组需要使用解热药的天数比例较低(27%[IQR 0-50] vs 50%[15-71];p=0.025)。与接受常规护理的参与者相比,随机分配接受布地奈德治疗的参与者在第 14 天和第 28 天有持续症状的比例较低(差异 0.204,95%CI 0.075 至 0.334;p=0.003)。在 14 天内,布地奈德组 CCQ 和 FLUPro 的总评分变化明显优于常规护理组(CCQ 平均差异 -0.12,95%CI -0.21 至 -0.02 [p=0.016];FLUPro 平均差异 -0.10,95%CI -0.21 至 -0.00 [p=0.044])。血氧饱和度和 SARS-CoV-2 载量(通过循环阈值测量)在两组之间无差异。布地奈德是安全的,只有 5 名(7%)参与者报告了自限性不良事件。
早期使用布地奈德吸入剂可降低需要紧急医疗护理的可能性,并缩短 COVID-19 轻症症状缓解后的康复时间。
国家卫生研究院生物医学研究中心和阿斯利康。