Functional, and Stereotactic Neurosurgery Service and Gamma Knife Unit, Assistance Publique - Hôpitaux de Marseille, Timone Hospital, Marseille, France.
Aix-Marseille University, Inserm, INS, Inst Neurosci Syst, Marseille, France.
Neurosurg Rev. 2021 Dec;44(6):3177-3188. doi: 10.1007/s10143-021-01528-y. Epub 2021 Apr 13.
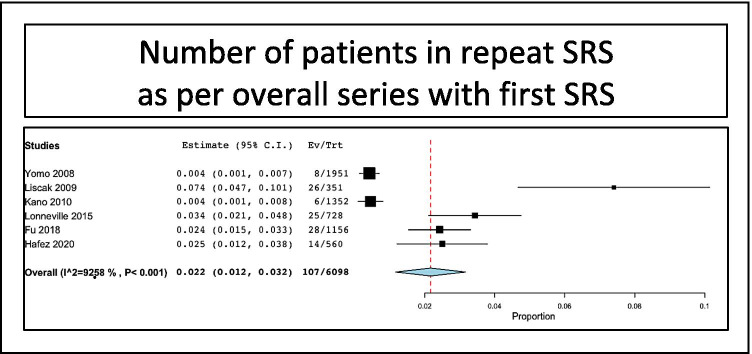
Vestibular schwannomas (VS) are slow-growing intracranial extraaxial benign tumors, developing from the vestibular part of the eight cranial nerves. Stereotactic radiosurgery (SRS) has now a long-term scientific track record as first intention treatment for small- to medium-sized VS. Though its success rate is very high, SRS for VS might fail to control tumor growth in some cases. However, the literature on repeat SRS after previously failed SRS remains scarce and reported in a low number of series with a limited number of cases. Here, we aimed at performing a systematic review and meta-analysis of the literature on repeat SRS for VS. Using PRISMA guidelines, we reviewed manuscripts published between January 1990 and October 2020 and referenced in PubMed. Tumor control and cranial nerve outcomes were evaluated with separate meta-analyses. Eight studies comprising 194 patients were included. The overall rate of patients treated in repeat SRS series as per overall series with first SRS was 2.2% (range 1.2-3.2%, p < 0.001). The mean time between first and second SRS was 50.7 months (median 51, range 44-64). The median marginal dose prescribed at first SRS was 12 Gy (range 8-24) and at second SRS was 12 Gy (range 9.8-19). After repeat SRS, tumor stability was reported in 61/194 patients, i.e., a rate of 29.6% (range 20.2-39%, I = 49.1%, p < 0.001). Tumor decrease was reported in 83/194 patients, i.e., a rate of 54.4% (range 33.7-75.1%, I = 89.1%, p < 0.001). Tumor progression was reported in 50/188 patients, i.e., a rate of 16.1% (range 2.5-29.7%, I = 87.1%, p = 0.02), rarely managed surgically. New trigeminal numbness was reported in 27/170 patients, i.e., a rate of 9.9% (range 1.4-18.3%, p < 0.02). New facial nerve palsy of worsened of previous was reported in 8/183 patients, i.e., a rate of 4.3% (range 1.4-7.2%, p = 0.004). Hearing loss was reported in 12/22 patients, i.e., a rate of 54.3% (range 24.8-83.8%, I = 70.7%, p < 0.001). Repeat SRS after previously failed SRS for VS is associated with high tumor control rates. Cranial nerve outcomes remain favorable, particularly for facial nerve. The rate of hearing loss appears similar to the one related to first SRS.
前庭神经鞘瘤(VS)是一种生长缓慢的颅内外轴良性肿瘤,起源于第八颅神经的前庭部分。立体定向放射外科(SRS)作为小至中等大小 VS 的首选治疗方法,已有长期的科学记录。尽管其成功率非常高,但在某些情况下,SRS 可能无法控制肿瘤生长。然而,关于先前 SRS 失败后重复 SRS 的文献仍然很少,并且在少数系列中报告,病例数量有限。在这里,我们旨在对先前 SRS 失败后重复 SRS 治疗 VS 的文献进行系统评价和荟萃分析。我们使用 PRISMA 指南,对 1990 年 1 月至 2020 年 10 月期间发表的文献进行了综述,并参考了 PubMed 中的文献。分别进行了荟萃分析评估肿瘤控制和颅神经结果。共纳入 8 项研究,包括 194 例患者。根据首次 SRS 的总系列,在重复 SRS 系列中接受治疗的患者的总比例为 2.2%(范围 1.2-3.2%,p<0.001)。首次和第二次 SRS 之间的平均时间为 50.7 个月(中位数 51,范围 44-64)。首次 SRS 时规定的边缘剂量中位数为 12 Gy(范围 8-24),第二次 SRS 时为 12 Gy(范围 9.8-19)。在重复 SRS 后,194 例患者中有 61 例报告肿瘤稳定,即 29.6%(范围 20.2-39%,I=49.1%,p<0.001)。报告肿瘤缩小的有 83 例患者,即 54.4%(范围 33.7-75.1%,I=89.1%,p<0.001)。报告肿瘤进展的有 50 例患者,即 16.1%(范围 2.5-29.7%,I=87.1%,p=0.02),很少需要手术治疗。170 例患者中有 27 例报告新出现三叉神经麻木,即 9.9%(范围 1.4-18.3%,p<0.02)。183 例患者中有 8 例报告新出现或恶化的面神经瘫痪,即 4.3%(范围 1.4-7.2%,p=0.004)。22 例患者中有 12 例报告听力损失,即 54.3%(范围 24.8-83.8%,I=70.7%,p<0.001)。先前 SRS 失败后重复 SRS 治疗 VS 与高肿瘤控制率相关。颅神经结果仍然良好,特别是面神经。听力损失的发生率似乎与首次 SRS 相关的发生率相似。