Lu Siyi, Liu Zhenzhen, Wang Bingyan, Li Fei, Meng Yan, Wang Junwei, Wang Yuxia, Wang Hao, Zhou Xin, Fu Wei
Department of General Surgery, Peking University Third Hospital, Beijing, 100191, China.
Department of Radiotherapy, Peking University Third Hospital, Beijing, 100191, China.
Cancer Cell Int. 2021 Apr 13;21(1):205. doi: 10.1186/s12935-021-01903-1.
Preoperative tumor markers, inflammation, and nutritional status are considered important predictors of prognosis and tumor response in locally advanced rectal cancer (LARC) patients. This study aims to explore the prognostic and predictive role of carcinoembryonic antigen (CEA), the Fibrinogen-Albumin Ratio Index (FARI), the Prognostic Nutritional Index (PNI) in LARC patients and compared them with a novel combined CEA-FARI-PNI (CFP) scoring system.
A total of 138 LARC patients undergoing radical surgery following neoadjuvant chemoradiotherapy (NCRT) between January 2012 and March 2019 were enrolled. The X-tile program was used to determine the optimal cut-off values of CEA, FARI, and PNI, and CFP scoring system was constructed accordingly. The prognostic ability of these factors was assessed by the time-dependent receiver operating characteristic (ROC) curve, Kaplan-Meier, Cox regression, and logistic regression. Nomogram was established to evaluate the predictive role of these factors in tumor response.
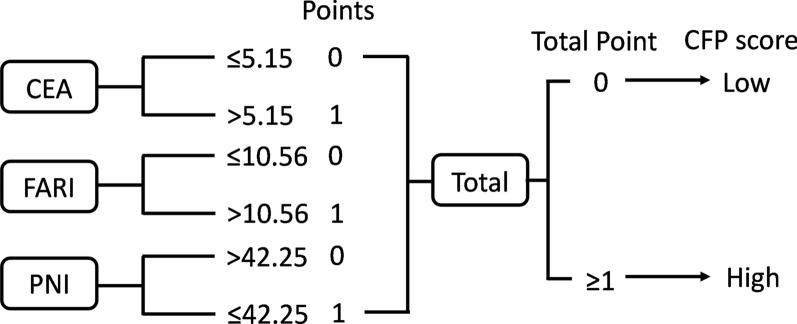
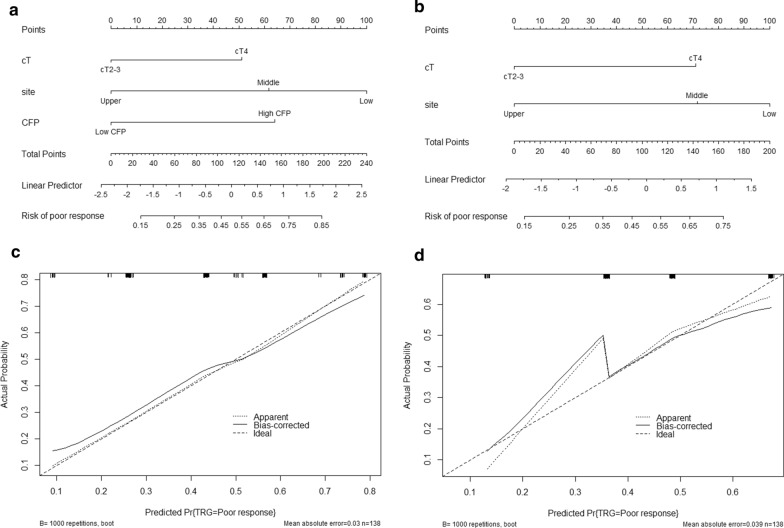
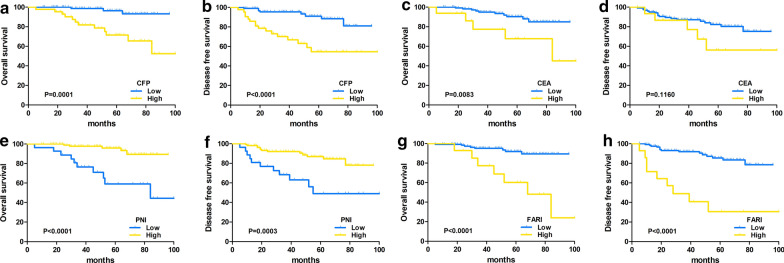
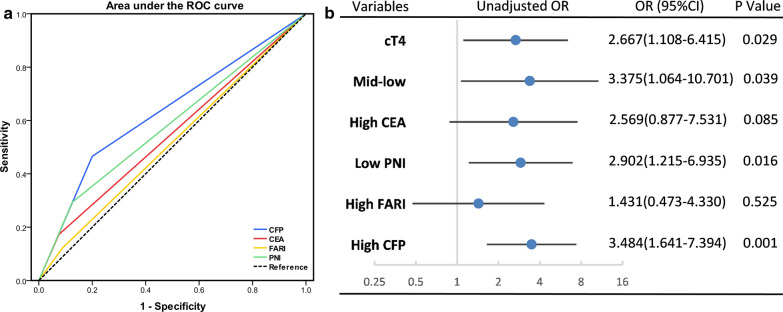
The optimal cut-off values of CEA, FARI, and PNI were 5.15 ng/l, 10.56%, and 42.25 g/L, respectively. The time-dependent ROC curve showed that compared to CEA, FARI, and PNI, CFP showed stable predictive efficacy for overall survival (OS) and disease-free survival (DFS). In multivariate analysis, CFP was the only factor that could independently predict OS (HR = 8.117, p = 0.001) and DFS (HR = 4.994, p < 0.001). Moreover, high CFP (OR = 3.693, p = 0.002) was also an independent risk factor of poor response. The area under the ROC curve (AUC) of the nomograms for predicting tumor response was better including CFP (0.717) than without CFP (0.656) (p < 0.05).
The CFP score was a more reliable marker for predicting OS, DFS, and NCRT efficacy in LARC patients, and the score could apparently improve predicted efficacy of the nomogram.
术前肿瘤标志物、炎症和营养状况被认为是局部晚期直肠癌(LARC)患者预后和肿瘤反应的重要预测指标。本研究旨在探讨癌胚抗原(CEA)、纤维蛋白原-白蛋白比率指数(FARI)、预后营养指数(PNI)在LARC患者中的预后和预测作用,并将它们与一种新的CEA-FARI-PNI(CFP)联合评分系统进行比较。
纳入2012年1月至2019年3月期间138例接受新辅助放化疗(NCRT)后行根治性手术的LARC患者。使用X-tile程序确定CEA、FARI和PNI的最佳临界值,并据此构建CFP评分系统。通过时间依赖性受试者操作特征(ROC)曲线、Kaplan-Meier法、Cox回归和逻辑回归评估这些因素的预后能力。建立列线图以评估这些因素在肿瘤反应中的预测作用。
CEA、FARI和PNI的最佳临界值分别为5.15 ng/l、10.56%和42.25 g/L。时间依赖性ROC曲线显示,与CEA、FARI和PNI相比,CFP对总生存期(OS)和无病生存期(DFS)具有稳定的预测效能。在多变量分析中,CFP是唯一能够独立预测OS(HR = 8.117,p = 0.001)和DFS(HR = 4.994,p < 0.001)的因素。此外,高CFP(OR = 3.693,p = 0.002)也是反应不佳的独立危险因素。预测肿瘤反应的列线图的ROC曲线下面积(AUC),纳入CFP时(0.717)比未纳入CFP时(0.656)更好(p < 0.05)。
CFP评分是预测LARC患者OS、DFS和NCRT疗效的更可靠标志物,该评分可明显提高列线图的预测效能。