Department of Medicine, Division of Nephrology, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, USA.
Department of Surgery, Massachusetts General Hospital, Boston, Massachusetts, USA.
J Immunother Cancer. 2021 Apr;9(4). doi: 10.1136/jitc-2020-002292.
Current guidelines for treatment of immune checkpoint inhibitor (ICI)-induced nephritis are not evidence based and may lead to excess corticosteroid exposure. We aimed to compare a rapid corticosteroid taper to standard of care.
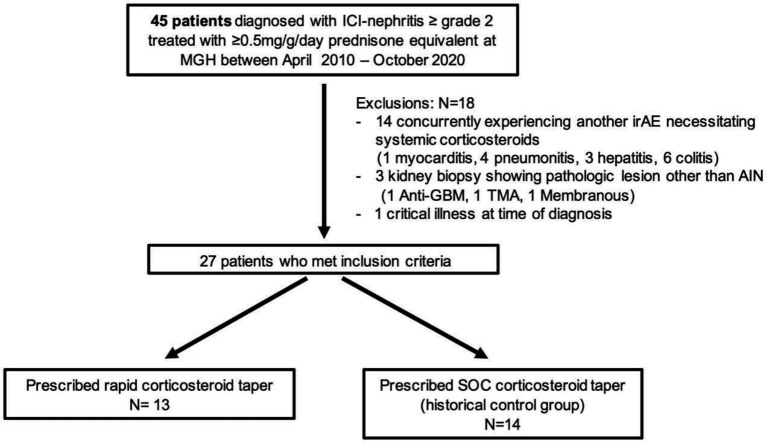
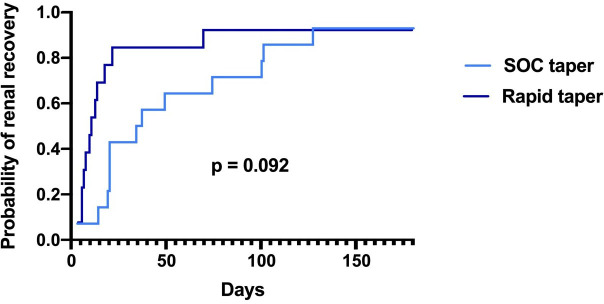
Retrospective cohort study in patients with ICI-induced nephritis comparing a rapid taper beginning with 60 mg/day prednisone and tapered to 10 mg within 3 weeks to a historical control group that began 60 mg/day tapered to 10 mg within 6 weeks (standard of care). Renal recovery was defined as creatinine returning to within 1.5-fold baseline. The log-rank test compared the differences in time to renal recovery between the groups. We report rates of renal recovery at 30, 60 and 90 days, and timing and outcomes of ICI rechallenge.
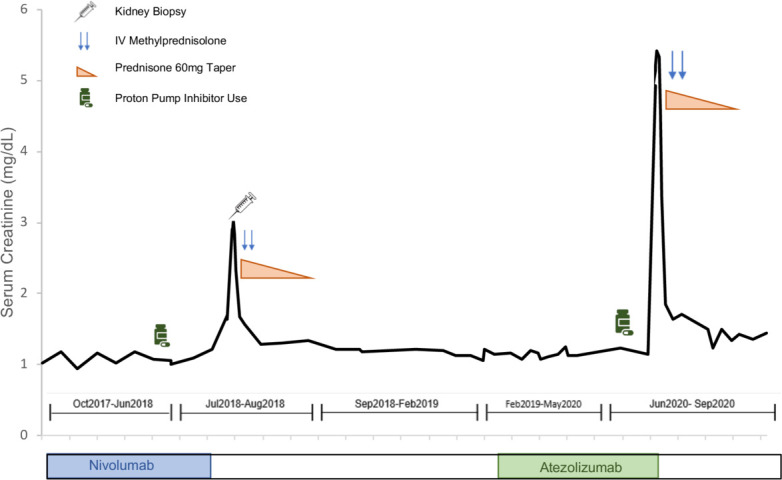
Thirteen patients received rapid corticosteroid taper and 14 patients received standard of care. Baseline characteristics were similar between groups. The median time to ≤10 mg/day prednisone was 20 days (IQR 15-25) in the rapid-taper group compared with 38 days (IQR 30-58) in the standard-of-care group. There was no significant difference in the time to renal recovery between the groups, though numerically higher numbers of patients recovered by 30 days, 11 (85%) in the rapid-taper arm versus 6 (46%) in the standard of care arm. Exposure to other nephritis-causing medications (proton pump inhibitor or trimethoprim-sulfamethoxazole) during the corticosteroid taper was more common in the standard of care group, 9 (64%) versus rapid-taper group, 2 (15%), and was associated with longer time to renal recovery, 20 days (IQR 14-101) versus 13 days (IQR 7-34) in those that discontinued nephritis-causing medications. Fifteen (56%) of patients were rechallenged with ICIs, and only two (13%) developed recurrent nephritis.
Patients with ICI-induced nephritis have excellent kidney outcomes when treated with corticosteroids that are tapered over 3 weeks.
目前针对免疫检查点抑制剂(ICI)诱导肾炎的治疗指南缺乏循证医学证据,可能导致皮质类固醇过度暴露。我们旨在比较快速皮质类固醇减量与标准治疗。
对ICI 诱导肾炎患者进行回顾性队列研究,比较起始剂量为 60mg/天泼尼松龙并在 3 周内快速减量至 10mg 的快速减量组与起始剂量为 60mg/天并在 6 周内减量至 10mg 的历史对照组(标准治疗)。肾脏恢复定义为肌酐恢复至基线的 1.5 倍以内。对数秩检验比较两组之间肾脏恢复时间的差异。我们报告了 30 天、60 天和 90 天的肾脏恢复率,以及 ICI 再挑战的时机和结果。
13 名患者接受了快速皮质类固醇减量,14 名患者接受了标准治疗。两组患者的基线特征相似。快速减量组中,泼尼松龙剂量降至≤10mg/天的中位数时间为 20 天(IQR 15-25),而标准治疗组为 38 天(IQR 30-58)。两组间肾脏恢复时间无显著差异,但在 30 天时有更多的患者恢复,快速减量组 11 例(85%),标准治疗组 6 例(46%)。在皮质类固醇减量期间,标准治疗组接受其他肾炎相关药物(质子泵抑制剂或甲氧苄啶-磺胺甲恶唑)治疗的患者更多,9 例(64%),而快速减量组为 2 例(15%),且与肾脏恢复时间较长相关,停药的患者为 20 天(IQR 14-101),未停药的患者为 13 天(IQR 7-34)。15 例(56%)患者再次接受 ICI 治疗,仅有 2 例(13%)出现复发性肾炎。
接受皮质类固醇治疗的 ICI 诱导肾炎患者肾脏结局良好,皮质类固醇减量时间为 3 周。