Negrea Lavinia, DeLozier Sarah J, Janes Jessica L, Rahman Mahboob, Dobre Mirela
Division of Nephrology and Hypertension, University Hospital Case Medical Center, Case Western Reserve University, Cleveland, OH.
University Hospitals Clinical Research Center, Cleveland, OH.
Kidney Med. 2021 Jan 12;3(2):183-192.e1. doi: 10.1016/j.xkme.2020.10.010. eCollection 2021 Mar-Apr.
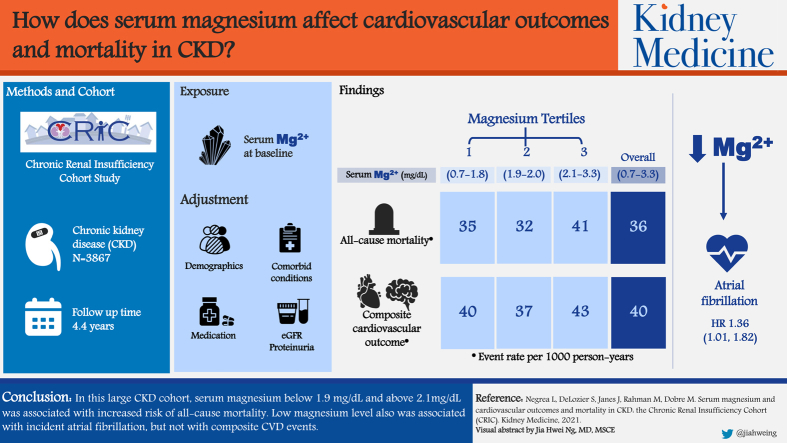
RATIONALE & OBJECTIVE: Low serum magnesium level has been shown to be associated with increased mortality, but its role as a predictor of cardiovascular disease is unclear. This study evaluates the association between serum magnesium level and cardiovascular events and all-cause mortality in a large cohort of individuals with chronic kidney disease (CKD).
Prospective cohort study.
SETTING & PARTICIPANTS: 3,867 participants with CKD, enrolled in the Chronic Renal Insufficiency Cohort (CRIC) Study.
Serum magnesium measured at study baseline.
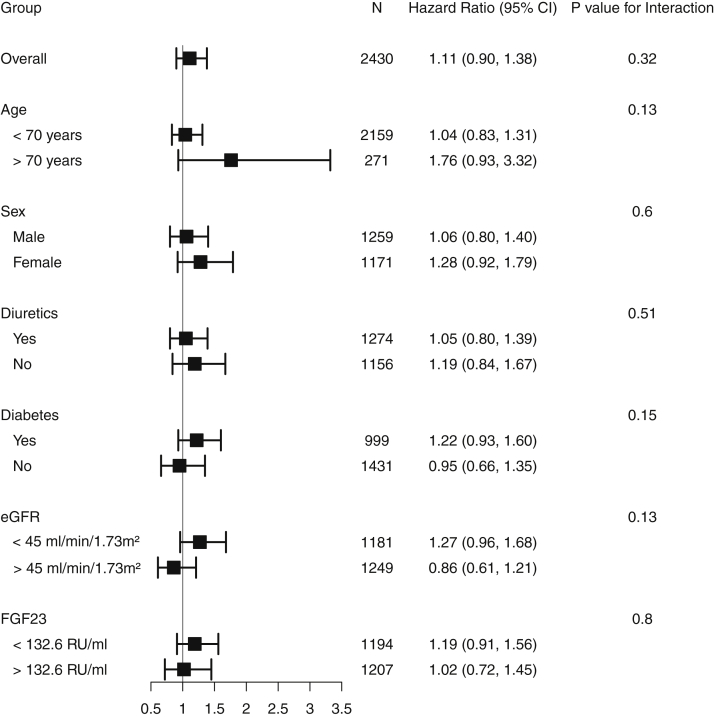
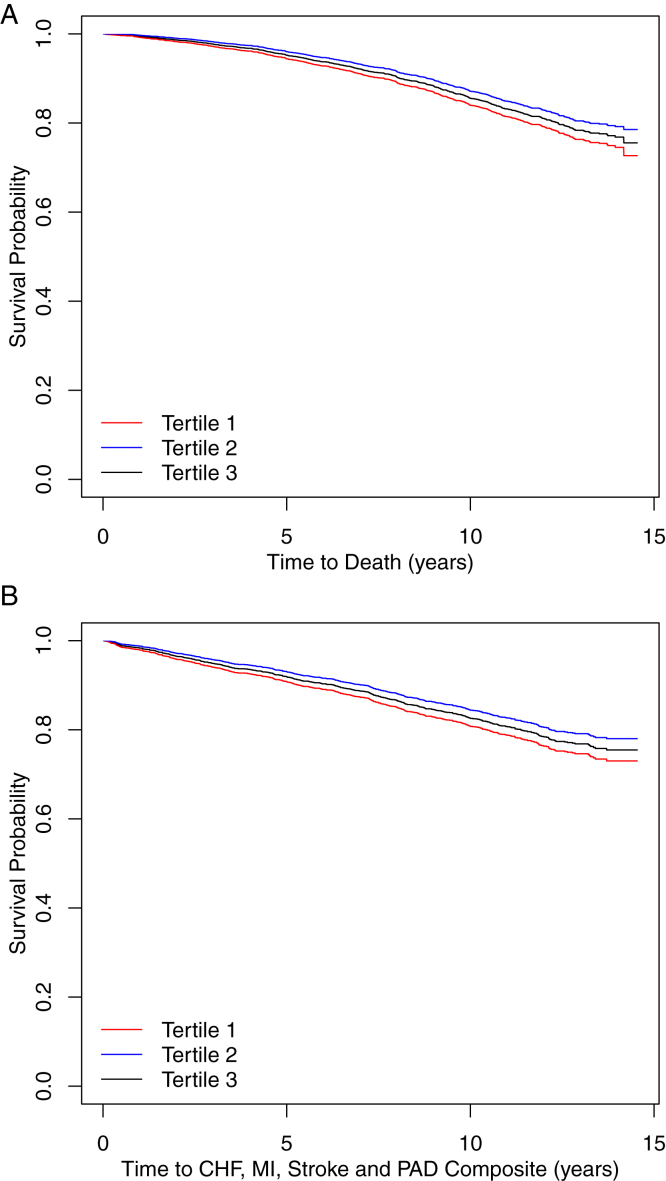
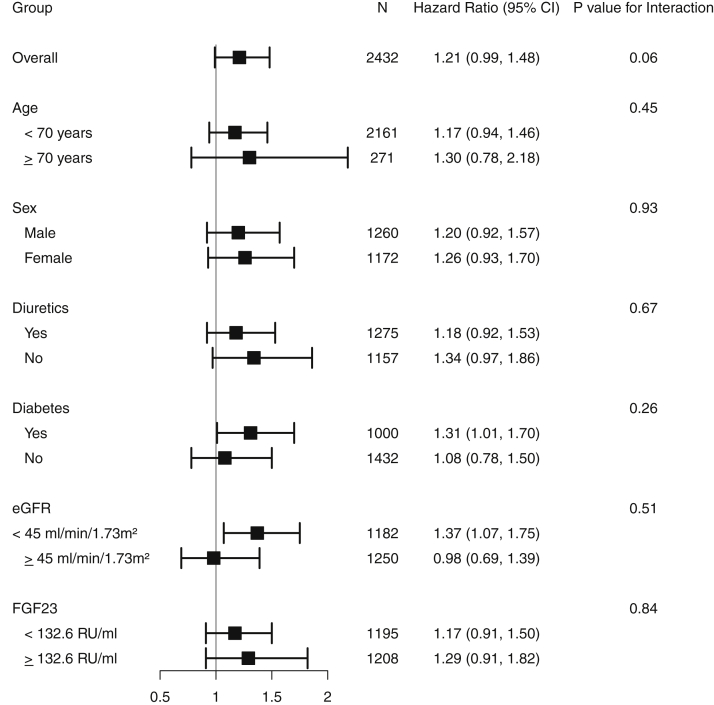
Composite cardiovascular events (myocardial infarction, cerebrovascular accident, heart failure, and peripheral arterial disease) and all-cause mortality.
Cox proportional hazards models adjusted for demographic, clinical, and laboratory characteristics.
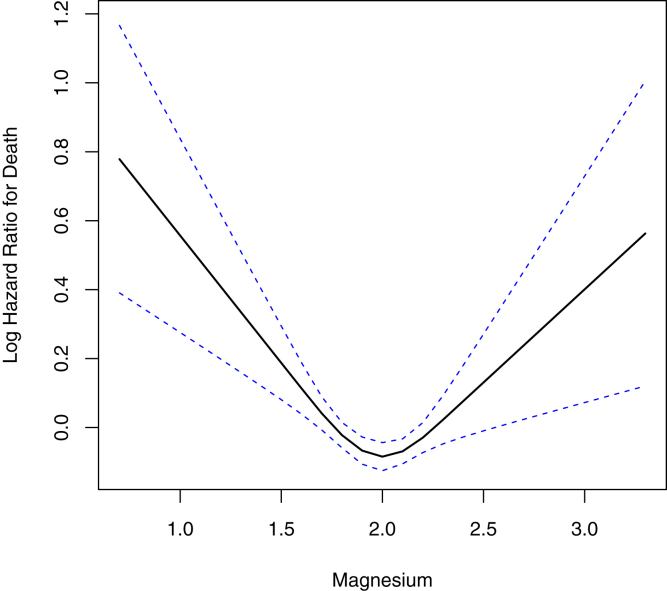
During the 14.6 (4.4) years (standard deviation) of follow-up, 1,384 participants died (36/1,000 person-years), and 1,227 (40/1,000 person-years) had a composite cardiovascular event. There was a nonlinear association between serum magnesium level and all-cause mortality. Low and high magnesium levels were associated with greater rates of all-cause mortality after adjusting for demographics, comorbid conditions, medications including diuretics, estimated glomerular filtration rate, and proteinuria ( < 0.001). No significant associations were observed between serum magnesium levels and the composite cardiovascular events. Low serum magnesium level was associated with incident atrial fibrillation (HR, 1.36; 95% CI, 1.01-1.82; = 0.04).
Single measurement of serum magnesium.
In this large CKD cohort, serum magnesium level < 1.9 mg/dL and >2.1 mg/dL was associated with increased risk for all-cause mortality. Low magnesium level was associated with incident atrial fibrillation but not with composite cardiovascular disease events. Further studies are needed to determine the optimal range of serum magnesium in CKD to prevent adverse clinical outcomes.
低血清镁水平已被证明与死亡率增加相关,但其作为心血管疾病预测指标的作用尚不清楚。本研究评估了一大群慢性肾脏病(CKD)患者的血清镁水平与心血管事件及全因死亡率之间的关联。
前瞻性队列研究。
3867名参与慢性肾功能不全队列(CRIC)研究的CKD患者。
研究基线时测量的血清镁。
复合心血管事件(心肌梗死、脑血管意外、心力衰竭和外周动脉疾病)及全因死亡率。
采用Cox比例风险模型,并对人口统计学、临床和实验室特征进行校正。
在14.6(4.4)年(标准差)的随访期间,1384名参与者死亡(36/1000人年),1227名(40/1000人年)发生复合心血管事件。血清镁水平与全因死亡率之间存在非线性关联。在校正人口统计学、合并症、包括利尿剂在内的药物、估计肾小球滤过率和蛋白尿后,低镁和高镁水平与更高的全因死亡率相关(P<0.001)。未观察到血清镁水平与复合心血管事件之间存在显著关联。低血清镁水平与新发房颤相关(HR,1.36;95%CI,1.01-1.82;P=0.04)。
血清镁单次测量。
在这个大型CKD队列中,血清镁水平<1.9mg/dL和>2.1mg/dL与全因死亡风险增加相关。低镁水平与新发房颤相关,但与复合心血管疾病事件无关。需要进一步研究以确定CKD患者血清镁的最佳范围,以预防不良临床结局。