Shah Rachana, Matthews Gregory J, Shah Rhia Y, McLaughlin Catherine, Chen Jing, Wolman Melanie, Master Stephen R, Chai Boyang, Xie Dawei, Rader Daniel J, Raj Dominic S, Mehta Nehal N, Budoff Matthew, Fischer Michael J, Go Alan S, Townsend Raymond R, He Jiang, Kusek John W, Feldman Harold I, Foulkes Andrea S, Reilly Muredach P
Division of Endocrinology and Diabetes, Children's Hospital of Philadelphia, Philadelphia, PA.
School of Public Health and Health Sciences, University of Massachusetts, Amherst, MA.
Am J Kidney Dis. 2015 Aug;66(2):266-73. doi: 10.1053/j.ajkd.2015.01.021. Epub 2015 Mar 17.
Cardiometabolic disease is a major cause of morbidity and mortality in persons with chronic kidney disease (CKD). Fractalkine (CX3CL1) is a potential mediator of both atherosclerosis and metabolic disease. Studies of the relationship of CX3CL1 with risk of cardiovascular disease (CVD) events and metabolic traits are lacking, particularly in the high-risk setting of CKD.
Cross-sectional and longitudinal observational analysis.
SETTING & PARTICIPANTS: Adults with CKD from 7 US sites participating in the Chronic Renal Insufficiency Cohort (CRIC) Study.
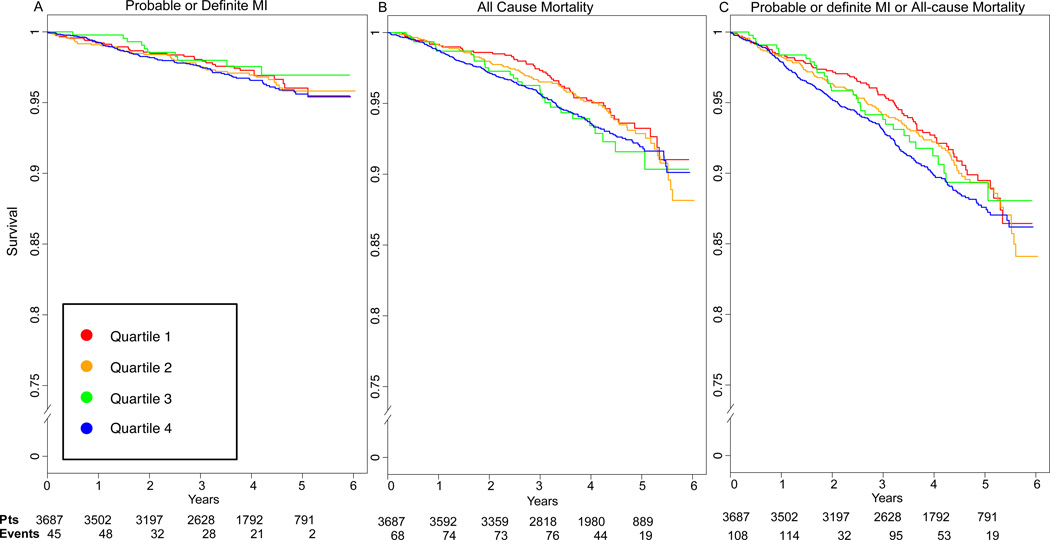
Quartiles of plasma CX3CL1 levels at baseline.
Baseline estimated glomerular filtration rate from a creatinine and cystatin C-based equation, prevalent and incident CVD, diabetes, metabolic syndrome and its criteria, homeostatic model assessment of insulin resistance, hemoglobin A1c level, myocardial infarction, all-cause mortality, and the composite outcome of myocardial infarction/all-cause mortality.
Among 3,687 participants, baseline CX3CL1 levels were associated positively with several CVD risk factors and metabolic traits, lower estimated glomerular filtration rate, and higher levels of inflammatory cytokines, as well as prevalent CVD (OR, 1.09; 95% CI, 1.01-1.19; P=0.03). Higher CX3CL1 level also was associated with prevalent diabetes (OR, 1.26; 95% CI, 1.16-1.38; P<0.001) in adjusted models. During a mean follow-up of 6 years, there were 352 deaths, 176 myocardial infarctions, and 484 composite outcomes. In fully adjusted models, 1-SD higher CX3CL1 level increased the hazard for all-cause mortality (1.11; 95% CI, 1.00-1.22; P=0.02) and the composite outcome (1.09; 95% CI, 1.00-1.19; P=0.04).
Study design did not allow evaluation of changes over time, correlation with progression of phenotypes, or determination of causality of effect.
Circulating CX3CL1 level may contribute to both atherosclerotic CVD and diabetes in a CKD cohort. Further studies are required to establish mechanisms through which CX3CL1 affects the pathogenesis of atherosclerosis and diabetes.
心脏代谢疾病是慢性肾脏病(CKD)患者发病和死亡的主要原因。趋化因子(CX3CL1)是动脉粥样硬化和代谢疾病的潜在介质。缺乏关于CX3CL1与心血管疾病(CVD)事件风险和代谢特征之间关系的研究,尤其是在CKD这种高危情况下。
横断面和纵向观察性分析。
来自美国7个地点的参与慢性肾功能不全队列(CRIC)研究的成年CKD患者。
基线时血浆CX3CL1水平的四分位数。
基于肌酐和胱抑素C的方程得出的基线估计肾小球滤过率、CVD的患病率和发病率、糖尿病、代谢综合征及其标准、胰岛素抵抗的稳态模型评估、糖化血红蛋白水平、心肌梗死、全因死亡率以及心肌梗死/全因死亡率的复合结局。
在3687名参与者中,基线CX3CL1水平与多种CVD危险因素和代谢特征、较低的估计肾小球滤过率以及较高水平的炎性细胞因子呈正相关,也与CVD患病率相关(比值比[OR],1.09;95%置信区间[CI],1.01 - 1.19;P = 0.03)。在调整模型中,较高的CX3CL1水平也与糖尿病患病率相关(OR,1.26;95% CI,1.16 - 1.38;P < 0.001)。在平均6年的随访期间,有352例死亡、176例心肌梗死和484例复合结局。在完全调整模型中,CX3CL1水平每升高1个标准差增加全因死亡率的风险(1.11;95% CI,1.00 - 1.22;P = 0.02)和复合结局的风险(1.09;95% CI,1.00 - 1.19;P = 0.04)。
研究设计不允许评估随时间的变化、与表型进展的相关性或效应因果关系的确定。
在CKD队列中,循环CX3CL1水平可能与动脉粥样硬化性CVD和糖尿病都有关。需要进一步研究以确定CX3CL1影响动脉粥样硬化和糖尿病发病机制的途径。