Division of Emergency Medicine, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, Illinois.
Department of Pediatrics, Northwestern University Feinberg School of Medicine, Chicago, Illinois.
JAMA Netw Open. 2021 Apr 1;4(4):e215832. doi: 10.1001/jamanetworkopen.2021.5832.
Bruising caused by physical abuse is the most common antecedent injury to be overlooked or misdiagnosed as nonabusive before an abuse-related fatality or near-fatality in a young child. Bruising occurs from both nonabuse and abuse, but differences identified by a clinical decision rule may allow improved and earlier recognition of the abused child.
To refine and validate a previously derived bruising clinical decision rule (BCDR), the TEN-4 (bruising to torso, ear, or neck or any bruising on an infant <4.99 months of age), for identifying children at risk of having been physically abused.
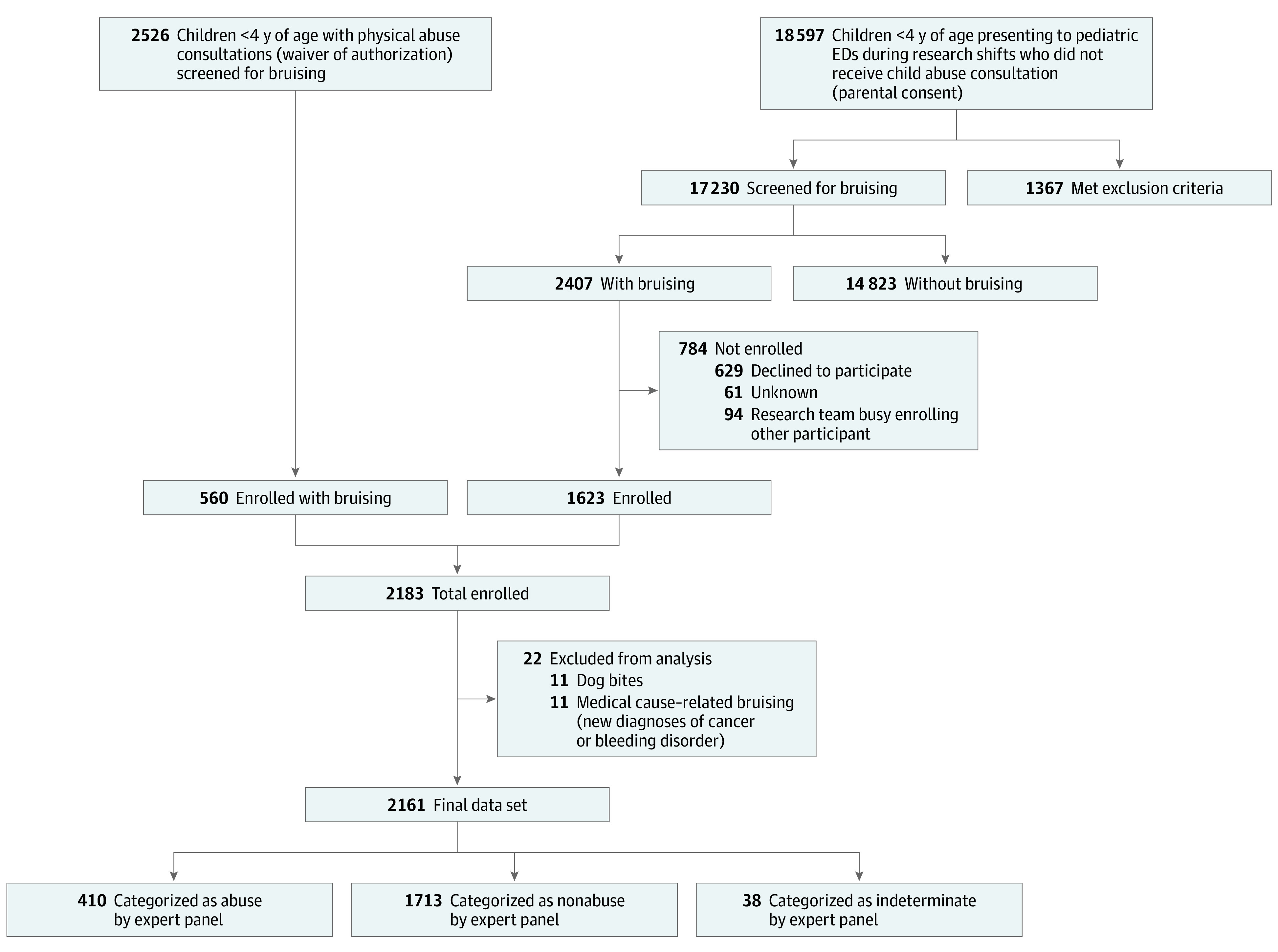
DESIGN, SETTING, AND PARTICIPANTS: This prospective cross-sectional study was conducted from December 1, 2011, to March 31, 2016, at emergency departments of 5 urban children's hospitals. Children younger than 4 years with bruising were identified through deliberate examination. Statistical analysis was completed in June 2020.
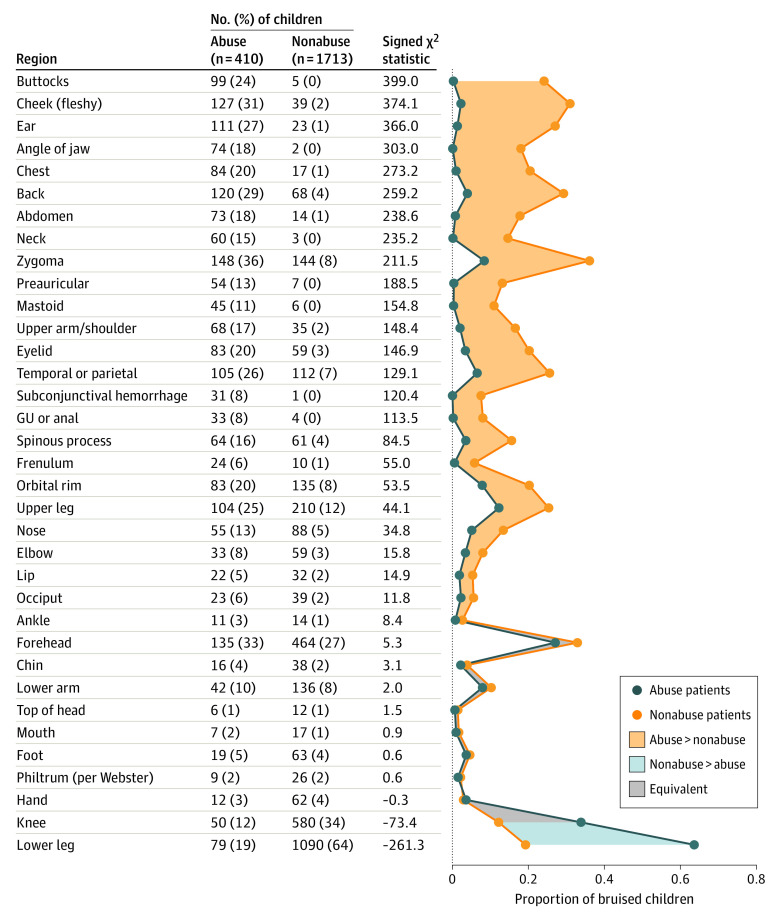
Bruising characteristics in 34 discrete body regions, patterned bruising, cumulative bruise counts, and patient's age. The BCDR was refined and validated based on these variables using binary recursive partitioning analysis.
Injury from abusive vs nonabusive trauma was determined by the consensus judgment of a multidisciplinary expert panel.
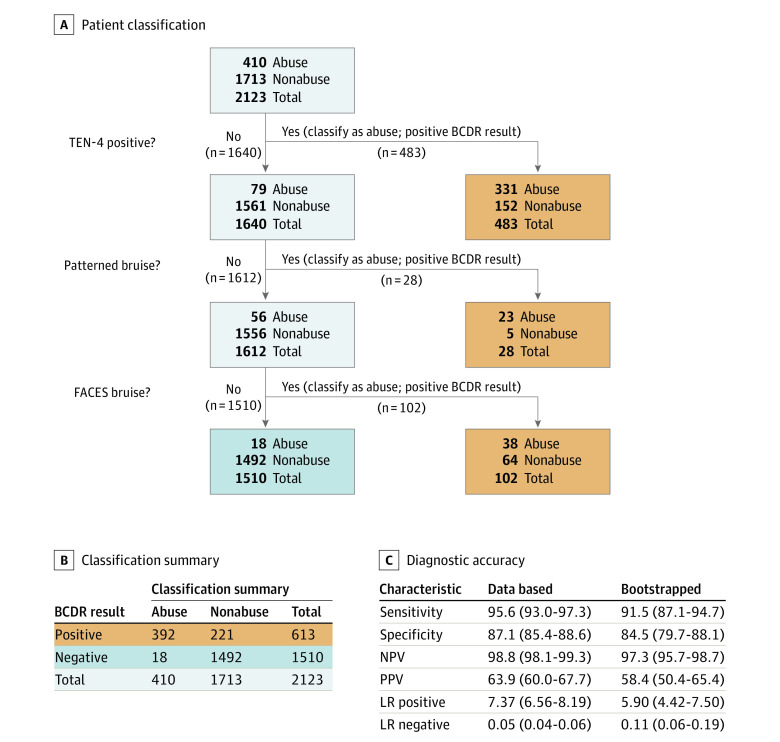
A total of 21 123 children were consecutively screened for bruising, and 2161 patients (mean [SD] age, 2.1 [1.1] years; 1296 [60%] male; 1785 [83%] White; 1484 [69%] non-Hispanic/Latino) were enrolled. The expert panel achieved consensus on 2123 patients (98%), classifying 410 (19%) as abuse and 1713 (79%) as nonabuse. A classification tree was fit to refine the rule and validated via bootstrap resampling. The resulting BCDR was 95.6% (95% CI, 93.0%-97.3%) sensitive and 87.1% (95% CI, 85.4%-88.6%) specific for distinguishing abuse from nonabusive trauma based on body region bruised (torso, ear, neck, frenulum, angle of jaw, cheeks [fleshy], eyelids, and subconjunctivae), bruising anywhere on an infant 4.99 months and younger, or patterned bruising (TEN-4-FACESp).
In this study, an affirmative finding for any of the 3 BCDR TEN-4-FACESp components in children younger than 4 years indicated a potential risk for abuse; these results warrant further evaluation. Clinical application of this tool has the potential to improve recognition of abuse in young children with bruising.
在幼儿虐待相关死亡或接近死亡之前,身体虐待引起的瘀伤是最常见的被忽视或误诊的既往损伤。瘀伤可由非虐待和虐待引起,但临床决策规则确定的差异可能有助于更早地识别受虐待的儿童。
改进和验证先前推导的瘀伤临床决策规则(BCDR),即 TEN-4(躯干、耳朵或颈部的瘀伤或任何 <4.99 个月大的婴儿的瘀伤),以识别有身体虐待风险的儿童。
设计、地点和参与者:这是一项从 2011 年 12 月 1 日至 2016 年 3 月 31 日在 5 家城市儿童医院急诊部门进行的前瞻性横断面研究。通过故意检查识别出 4 岁以下有瘀伤的儿童。统计分析于 2020 年 6 月完成。
34 个离散身体部位的瘀伤特征、模式性瘀伤、累积瘀伤计数和患者年龄。BCDR 是基于这些变量使用二元递归分割分析进行改进和验证的。
滥用与非滥用创伤造成的损伤由多学科专家小组的共识判断确定。
共对 21123 名儿童进行了连续筛查瘀伤,共纳入 2161 名患者(平均[标准差]年龄 2.1[1.1]岁;1296[60%]男性;1785[83%]白人;1484[69%]非西班牙裔/拉丁裔)。专家组就 2123 名患者(98%)达成共识,将 410 名(19%)归类为虐待,将 1713 名(79%)归类为非虐待。拟合分类树以改进规则,并通过引导重采样进行验证。由此产生的 BCDR 在区分身体区域瘀伤(躯干、耳朵、颈部、系带、下颌角、脸颊[肉质]、眼睑和眼结膜下)、任何地方瘀伤在 4.99 个月及以下的婴儿或模式性瘀伤(TEN-4-FACESp)时,对区分虐待和非虐待创伤的敏感度为 95.6%(95%CI,93.0%-97.3%),特异性为 87.1%(95%CI,85.4%-88.6%)。
在这项研究中,4 岁以下儿童任何 BCDR TEN-4-FACESp 成分呈阳性均表明存在潜在的虐待风险;这些结果值得进一步评估。该工具的临床应用有可能改善对有瘀伤的幼儿虐待的识别。