Fellahi Jean-Luc, Futier Emmanuel, Vaisse Camille, Collange Olivier, Huet Olivier, Loriau Jerôme, Gayat Etienne, Tavernier Benoit, Biais Matthieu, Asehnoune Karim, Cholley Bernard, Longrois Dan
Service D'Anesthésie-Réanimation, Hôpital Louis Pradel, 59 boulevard Pinel, 69500, Hospices Civils de Lyon, Lyon, France.
Laboratoire CarMeN, Université Claude Bernard Lyon 1, Inserm U1060, Lyon, France.
Ann Intensive Care. 2021 Apr 14;11(1):58. doi: 10.1186/s13613-021-00845-1.
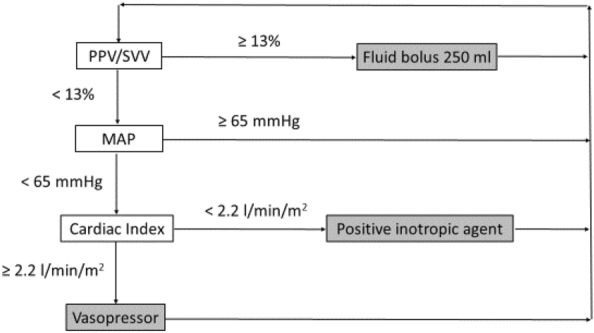
Despite a large body of evidence, the implementation of guidelines on hemodynamic optimization and goal-directed therapy remains limited in daily routine practice. To facilitate/accelerate this implementation, a panel of experts in the field proposes an approach based on six relevant questions/answers that are frequently mentioned by clinicians, using a critical appraisal of the literature and a modified Delphi process. The mean arterial pressure is a major determinant of organ perfusion, so that the authors unanimously recommend not to tolerate absolute values below 65 mmHg during surgery to reduce the risk of postoperative organ dysfunction. Despite well-identified limitations, the authors unanimously propose the use of dynamic indices to rationalize fluid therapy in a large number of patients undergoing non-cardiac surgery, pending the implementation of a "validity criteria checklist" before applying volume expansion. The authors recommend with a good agreement mini- or non-invasive stroke volume/cardiac output monitoring in moderate to high-risk surgical patients to optimize fluid therapy on an individual basis and avoid volume overload. The authors propose to use fluids and vasoconstrictors in combination to achieve optimal blood flow and maintain perfusion pressure above the thresholds considered at risk. Although purchase of disposable sensors and stand-alone monitors will result in additional costs, the authors unanimously acknowledge that there are data strongly suggesting this may be counterbalanced by a sustained reduction in postoperative morbidity and hospital lengths of stay. Beside existing guidelines, knowledge and explicit clinical reasoning tools followed by decision algorithms are mandatory to implement individualized hemodynamic optimization strategies and reduce postoperative morbidity and duration of hospital stay in high-risk surgical patients.
尽管有大量证据,但血流动力学优化和目标导向治疗指南在日常临床实践中的实施仍然有限。为了促进/加速这一实施,该领域的一组专家提出了一种基于临床医生经常提到的六个相关问题/答案的方法,采用文献的批判性评价和改进的德尔菲法。平均动脉压是器官灌注的主要决定因素,因此作者一致建议在手术期间不要容忍绝对值低于65 mmHg,以降低术后器官功能障碍的风险。尽管存在明确的局限性,但作者一致建议在大量接受非心脏手术的患者中使用动态指标来合理进行液体治疗,在进行容量扩充之前先实施“有效性标准清单”。作者强烈建议对中高危手术患者进行微创或无创每搏量/心输出量监测,以个体化优化液体治疗并避免容量超负荷。作者建议联合使用液体和血管收缩剂,以实现最佳血流并将灌注压维持在有风险的阈值以上。尽管购买一次性传感器和独立监测仪会产生额外成本,但作者一致承认,有数据强烈表明,这可能会被术后发病率和住院时间的持续缩短所抵消。除了现有的指南外,知识和明确的临床推理工具以及决策算法对于实施个体化血流动力学优化策略以及降低高危手术患者的术后发病率和住院时间至关重要。