Silva D L, Lima C M, Magalhães V C R, Baltazar L M, Peres N T A, Caligiorne R B, Moura A S, Fereguetti T, Martins J C, Rabelo L F, Abrahão J S, Lyon A C, Johann S, Santos D A
Department of Microbiology, Institute of Biological Sciences, Universidade Federal de Minas Gerais, Belo Horizonte, Minas Gerais, Brazil.
Department of Microbiology, Institute of Biological Sciences, Universidade Federal de Minas Gerais, Belo Horizonte, Minas Gerais, Brazil; Hospital Eduardo de Menezes, Fundação Hospitalar do Estado de Minas Gerais (FHEMIG), Belo Horizonte, Minas Gerais, Brazil.
J Hosp Infect. 2021 Jul;113:145-154. doi: 10.1016/j.jhin.2021.04.001. Epub 2021 Apr 20.
SARS-CoV-2 predisposes patients to secondary infections; however, a better understanding of the impact of coinfections on the outcome of hospitalized COVID-19 patients is still necessary.
To analyse death risk due to coinfections in COVID-19 patients.
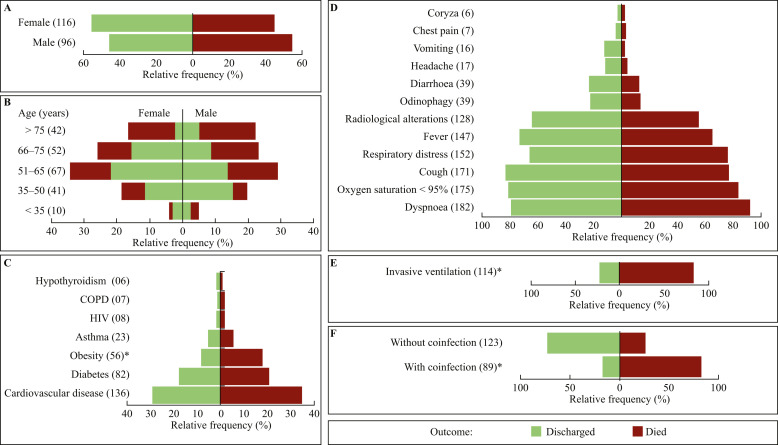
The odds of death of 212 severely ill COVID-19 patients were evaluated, with detailed focus on the risks for each pathogen, site of infection, comorbidities and length of hospitalization.
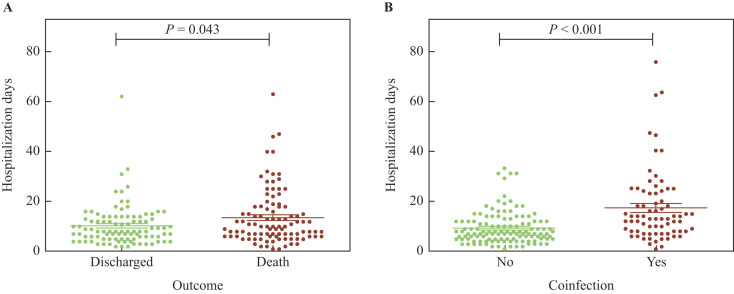
The mortality rate was 50.47%. Fungal and/or bacterial isolation occurred in 89 patients, of whom 83.14% died. Coinfected patients stayed hospitalized longer and had an increased odds of dying (odds ratio (OR): 13.45; R = 0.31). The risk of death was increased by bacterial (OR: 11.28) and fungal (OR: 5.97) coinfections, with increased levels of creatinine, leucocytes, urea and C-reactive protein. Coinfections increased the risk of death if patients suffered from cardiovascular disease (OR: 11.53), diabetes (OR: 6.00) or obesity (OR: 5.60) in comparison with patients with these comorbidities but without pathogen isolation. The increased risk of death was detected for coagulase-negative Staphylococcus (OR: 25.39), Candida non-albicans (OR: 11.12), S. aureus (OR: 10.72), Acinetobacter spp. (OR: 6.88), Pseudomonas spp. (OR: 4.77), and C. albicans (OR: 3.97). The high-risk sites of infection were blood, tracheal aspirate, and urine. Patients with coinfection undergoing invasive mechanical ventilation were 3.8 times more likely to die than those without positive cultures.
Severe COVID-19 patients with secondary coinfections required longer hospitalization and had higher risk of death. The early diagnosis of coinfections is essential to identify high-risk patients and to determine the right interventions to reduce mortality.
严重急性呼吸综合征冠状病毒2(SARS-CoV-2)使患者易发生继发感染;然而,仍有必要更好地了解合并感染对住院的2019冠状病毒病(COVID-19)患者预后的影响。
分析COVID-19患者合并感染导致的死亡风险。
评估了212例重症COVID-19患者的死亡几率,详细关注每种病原体的风险、感染部位、合并症和住院时间。
死亡率为50.47%。89例患者分离出真菌和/或细菌,其中83.14%死亡。合并感染的患者住院时间更长,死亡几率增加(优势比(OR):13.45;R = 0.31)。细菌(OR:11.28)和真菌(OR:5.97)合并感染会增加死亡风险,同时肌酐、白细胞、尿素和C反应蛋白水平升高。与有这些合并症但无病原体分离的患者相比,如果患者患有心血管疾病(OR:11.53)、糖尿病(OR:6.00)或肥胖症(OR:5.60),合并感染会增加死亡风险。检测到凝固酶阴性葡萄球菌(OR:25.39)、非白色念珠菌(OR:11.12)、金黄色葡萄球菌(OR:10.72)、不动杆菌属(OR:6.88)、假单胞菌属(OR:4.77)和白色念珠菌(OR:3.97)的死亡风险增加。感染的高危部位是血液、气管吸出物和尿液。接受有创机械通气的合并感染患者死亡的可能性是培养结果为阴性患者的3.8倍。
继发合并感染的重症COVID-19患者需要更长的住院时间,死亡风险更高。合并感染的早期诊断对于识别高危患者和确定正确的干预措施以降低死亡率至关重要。