Division of Infectious Diseases, Department of Medicine, Bryn Mawr Hospital, Main Line Health System, Bryn Mawr, PA, USA.
Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, PA, USA.
Ann Clin Microbiol Antimicrob. 2021 Sep 25;20(1):69. doi: 10.1186/s12941-021-00472-5.
Coronavirus SARS-CoV-2 causes COVID-19 illness which can progress to severe pneumonia. Empiric antibacterials are often employed though frequency of bacterial coinfection superinfection is debated and concerns raised about selection of bacterial antimicrobial resistance. We evaluated sputum bacterial and fungal growth from 165 intubated COVID-19 pneumonia patients. Objectives were to determine frequency of culture positivity, risk factors for and outcomes of positive cultures, and timing of antimicrobial resistance development.
Retrospective reviews were conducted of COVID-19 pneumonia patients requiring intubation admitted to a 1058-bed four community hospital system on the east coast United States, March 1 to May 1, 2020. Length of stay (LOS) was expressed as mean (standard deviation); 95% confidence interval (95% CI) was computed for overall mortality rate using the exact binomial method, and overall mortality was compared across each level of a potential risk factor using a Chi-Square Test of Independence. All tests were two-sided, and significance level was set to 0.05.
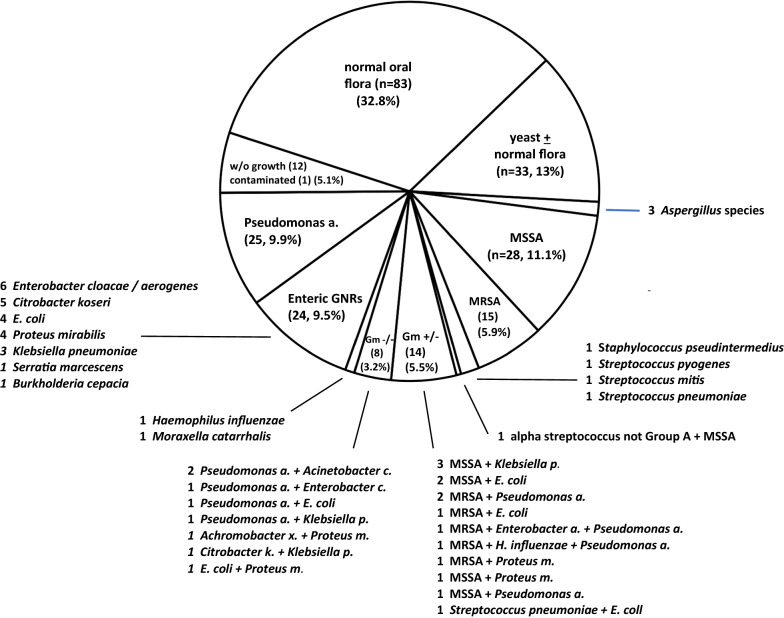
Average patient age was 68.7 years and LOS 19.9 days. Eighty-three patients (50.3% of total) originated from home, 10 from group homes (6.1% of total), and 72 from nursing facilities (43.6% of total). Mortality was 62.4%, highest for nursing home residents (80.6%). Findings from 253 sputum cultures overall did not suggest acute bacterial or fungal infection in 73 (45%) of 165 individuals sampled within 24 h of intubation. Cultures ≥ 1 week following intubation did grow potential pathogens in 72 (64.9%) of 111 cases with 70.8% consistent with late pneumonia and 29.2% suggesting colonization. Twelve (10.8% of total) of these late post-intubation cultures revealed worsened antimicrobial resistance predominantly in Pseudomonas, Enterobacter, or Staphylococcus aureus.
In severe COVID-19 pneumonia, a radiographic ground glass interstitial pattern and lack of purulent sputum prior to/around the time of intubation correlated with no culture growth or recovery of normal oral flora ± yeast. Discontinuation of empiric antibacterials should be considered in these patients aided by other clinical findings, history of prior antimicrobials, laboratory testing, and overall clinical course. Continuing longterm hospitalisation and antibiotics are associated with sputum cultures reflective of hospital-acquired microbes and increasing antimicrobial resistance.
Not applicable as this was a retrospective chart review study without interventional arm.
冠状病毒 SARS-CoV-2 会引起 COVID-19 疾病,这种疾病可能会发展成严重肺炎。经验性使用抗菌药物是很常见的,尽管细菌合并感染的频率存在争议,而且人们对细菌对抗菌药物耐药性的选择表示担忧。我们评估了 165 例气管插管 COVID-19 肺炎患者的痰液细菌和真菌生长情况。目的是确定培养阳性的频率、阳性培养的危险因素和结果,以及抗菌药物耐药性发展的时间。
对 2020 年 3 月 1 日至 5 月 1 日在美国东海岸一家拥有 1058 张床位的四家社区医院系统中需要插管的 COVID-19 肺炎患者进行回顾性研究。住院时间(LOS)用平均值(标准差)表示;使用精确二项式法计算总死亡率的 95%置信区间(95%CI),并使用卡方检验独立性比较每个潜在危险因素水平的总死亡率。所有检验均为双侧检验,显著性水平设定为 0.05。
患者平均年龄为 68.7 岁,住院时间为 19.9 天。83 例(总数的 50.3%)来自家庭,10 例(总数的 6.1%)来自团体之家,72 例(总数的 43.6%)来自护理院。死亡率为 62.4%,其中护理院居民最高(80.6%)。253 份痰培养的结果表明,在插管后 24 小时内取样的 165 名患者中,有 73 名(45%)未出现急性细菌或真菌感染。在插管后 1 周以上的培养物中,111 例中有 72 例(64.9%)生长出潜在病原体,其中 70.8%与晚期肺炎一致,29.2%提示定植。在这些晚期插管后培养物中,有 12 例(总病例的 10.8%)显示出抗菌药物耐药性恶化,主要是铜绿假单胞菌、肠杆菌或金黄色葡萄球菌。
在严重的 COVID-19 肺炎中,在插管前/插管时存在放射学磨玻璃间质模式和无脓性痰与无培养物生长或恢复正常口腔菌群(±酵母)相关。应根据其他临床发现、先前使用抗菌药物的病史、实验室检测和整体临床病程,考虑停止经验性使用抗菌药物。长期住院和使用抗生素与反映医院获得性微生物和抗菌药物耐药性增加的痰培养有关。
由于这是一项没有干预组的回顾性图表审查研究,因此不适用。