Clarsen Benjamin, Skogen Jens Christoffer, Nilsen Thomas Sevenius, Aarø Leif Edvard
Department of Health Promotion, Norwegian Institute of Public Health, Zander Kaaes Gate, 5017, Bergen, Norway.
Oslo Sports Trauma Research Centre, Norwegian School of Sport Sciences, Oslo, Norway.
BMC Public Health. 2021 Apr 15;21(1):730. doi: 10.1186/s12889-021-10764-2.
The continuum of resistance model's premise is that delayed respondents to a survey are more similar to non-respondents than early respondents are. For decades, survey researchers have applied this model in attempts to evaluate and adjust for non-response bias. Despite a recent resurgence in the model's popularity, its value has only been assessed in one large online population health survey.
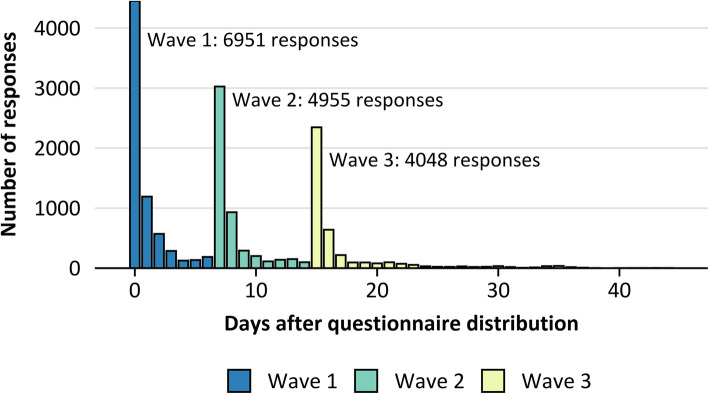
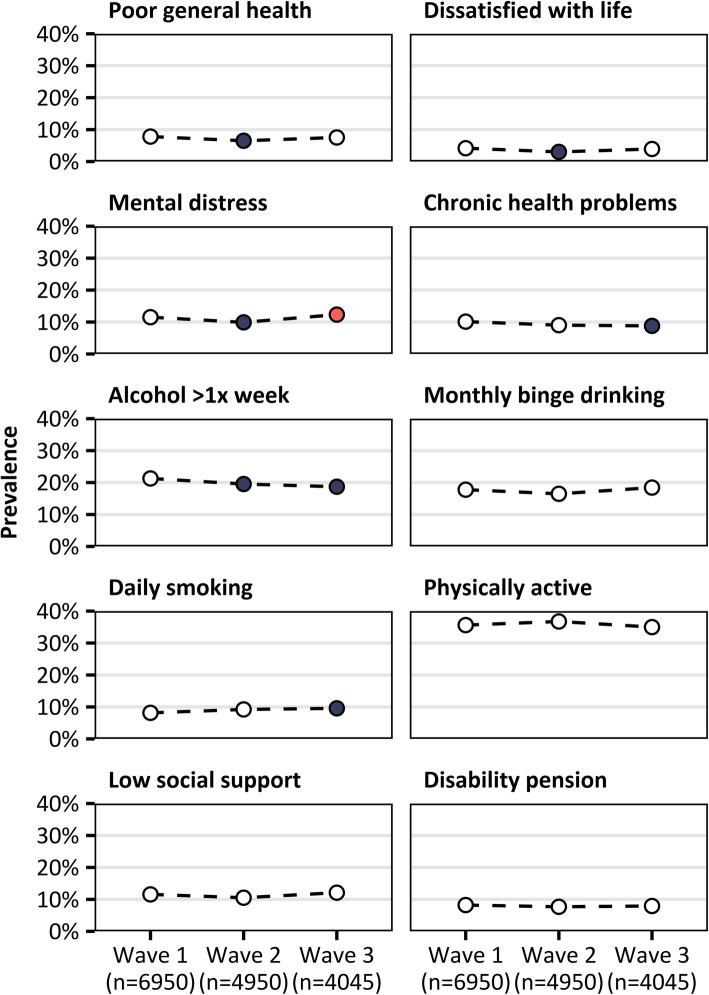
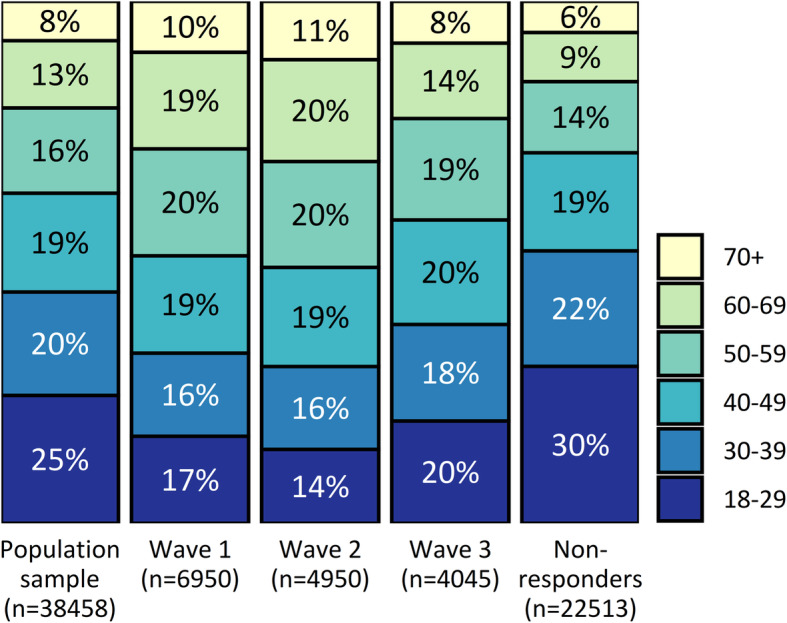
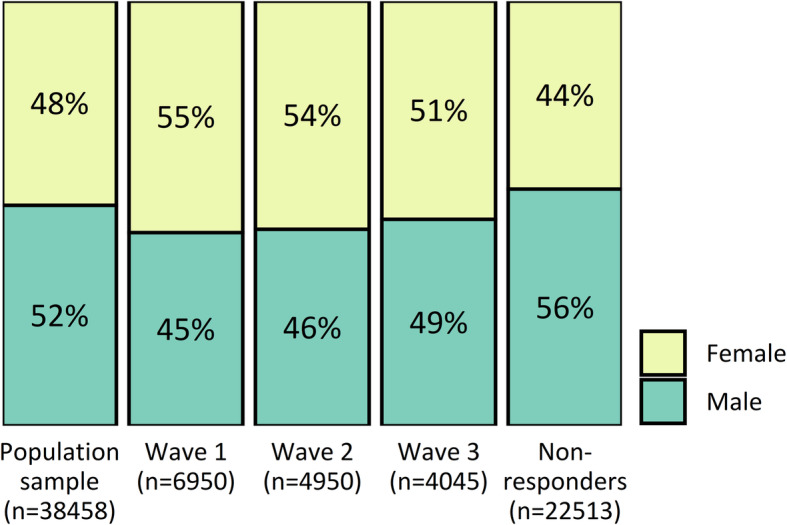
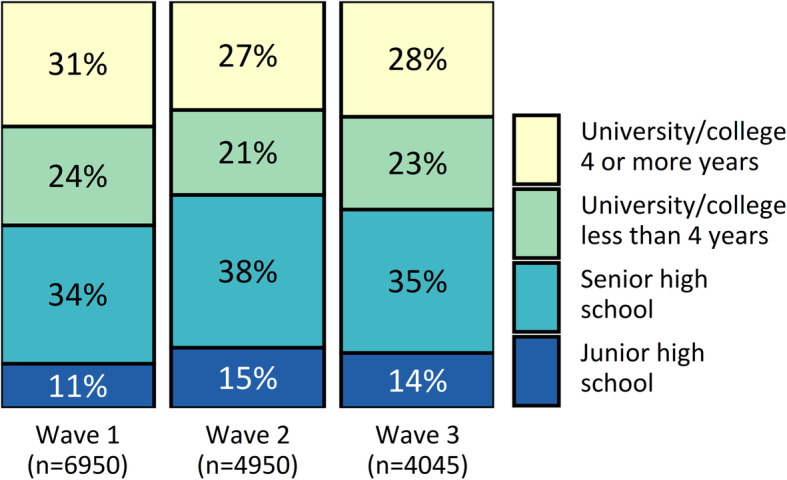
Respondents to the Norwegian Counties Public Health Survey in Hordaland, Norway, were divided into three groups: those who responded within 7 days of the initial email/SMS invitation (wave 1, n = 6950); those who responded after 8 to 14 days and 1 reminder (wave 2, n = 4950); and those who responded after 15 or more days and 2 reminders (wave 3, n = 4045). Logistic regression analyses were used to compare respondents' age, sex and educational level between waves, as well as the prevalence of poor general health, life dissatisfaction, mental distress, chronic health problems, weekly alcohol consumption, monthly binge drinking, daily smoking, physical activity, low social support and receipt of a disability pension.
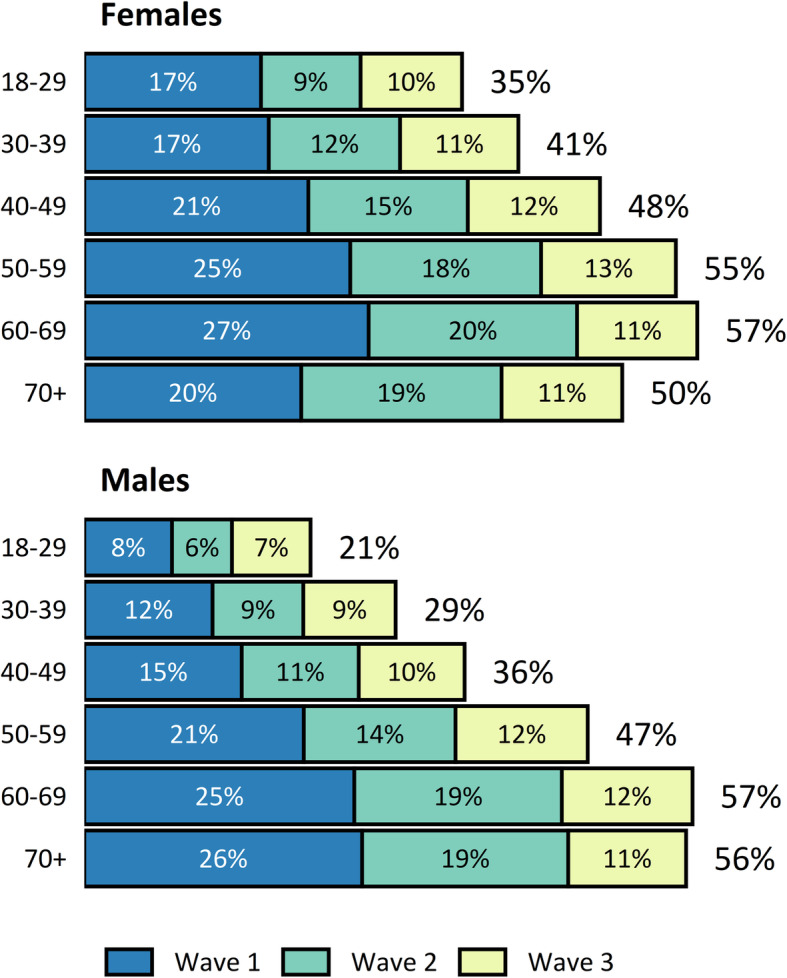
The overall response to the survey was 41.5%. Respondents in wave 1 were more likely to be older, female and more highly educated than those in waves 2 and 3. However, there were no substantial differences between waves for any health outcomes, with a maximal prevalence difference of 2.6% for weekly alcohol consumption (wave 1: 21.3%, wave 3: 18.7%).
There appeared to be a mild continuum of resistance for demographic variables. However, this was not reflected in health and related outcomes, which were uniformly similar across waves. The continuum of resistance model is unlikely to be useful to adjust for nonresponse bias in large online surveys of population health.
抗性连续体模型的前提是,调查中的延迟受访者与未受访者比早期受访者更为相似。几十年来,调查研究人员一直应用该模型来评估和调整无应答偏差。尽管该模型最近再度流行,但其价值仅在一项大型在线人群健康调查中得到评估。
挪威霍达兰郡公共卫生调查的受访者被分为三组:在首次电子邮件/短信邀请后7天内回复的受访者(第1波,n = 6950);在8至14天并收到1次提醒后回复的受访者(第2波,n = 4950);以及在15天或更长时间并收到2次提醒后回复的受访者(第3波,n = 4045)。采用逻辑回归分析比较各波受访者的年龄、性别和教育水平,以及总体健康状况差、生活不满意、精神困扰、慢性健康问题、每周饮酒量、每月暴饮、每日吸烟、体育活动、社会支持低和领取残疾抚恤金的患病率。
该调查的总体回复率为41.5%。第1波受访者比第2波和第3波受访者更有可能年龄较大、为女性且受教育程度更高。然而,各波在任何健康结果方面均无实质性差异,每周饮酒量的最大患病率差异为2.6%(第1波:21.3%,第3波:18.7%)。
人口统计学变量似乎存在轻度的抗性连续体。然而,这并未反映在健康及相关结果中,各波结果均相似。抗性连续体模型不太可能用于调整大型在线人群健康调查中的无应答偏差。