Population Health Unit, KEMRI-Wellcome Trust Research Programme, Nairobi, Kenya
Population Health Unit, KEMRI-Wellcome Trust Research Programme, Nairobi, Kenya.
BMJ Glob Health. 2021 Apr;6(4). doi: 10.1136/bmjgh-2020-004544.
To improve child survival, it is necessary to describe and understand the spatial and temporal variation of factors associated with child survival beyond national aggregates, anchored at decentralised health planning units. Therefore, we aimed to provide subnational estimates of factors associated with child survival while elucidating areas of progress, stagnation and decline in Kenya.
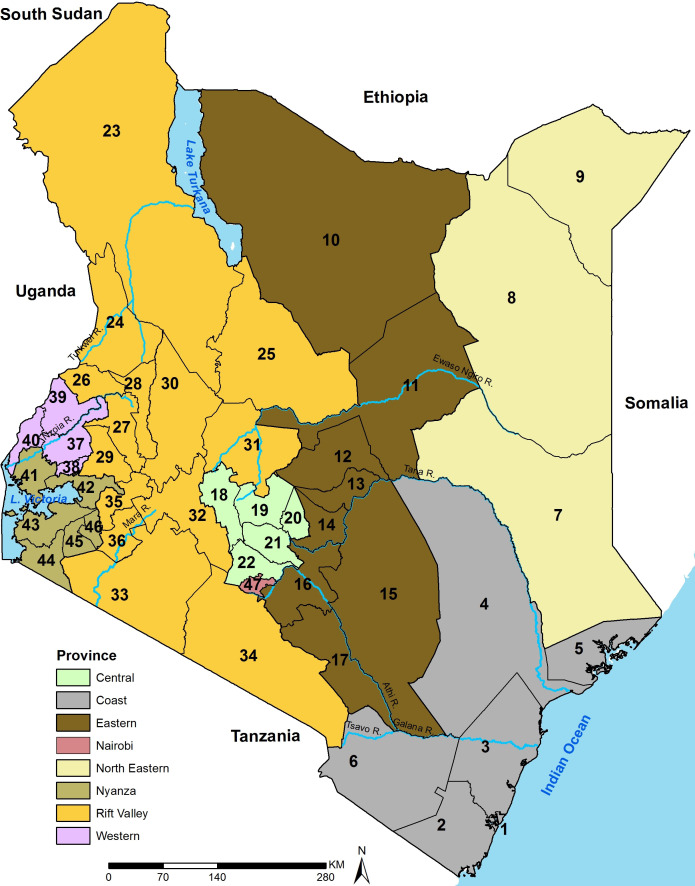
Twenty household surveys and three population censuses conducted since 1989 were assembled and spatially aligned to 47 subnational Kenyan county boundaries. Bayesian spatio-temporal Gaussian process regression models accounting for inadequate sample size and spatio-temporal relatedness were fitted for 43 factors at county level between 1993 and 2014.
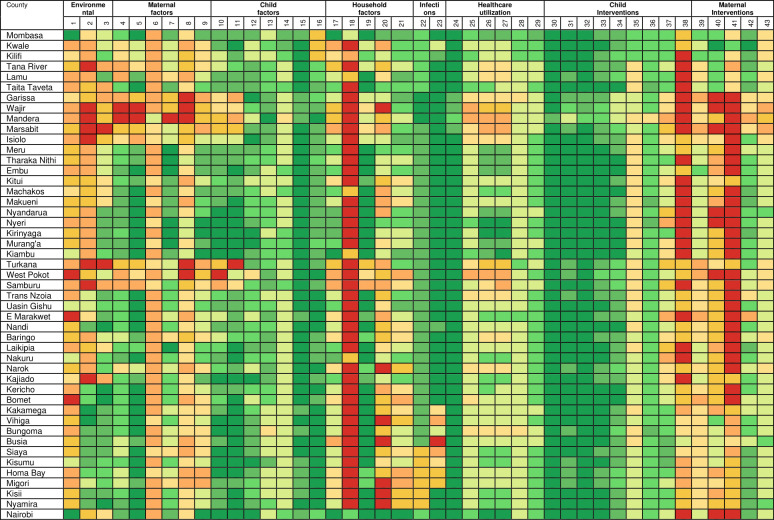
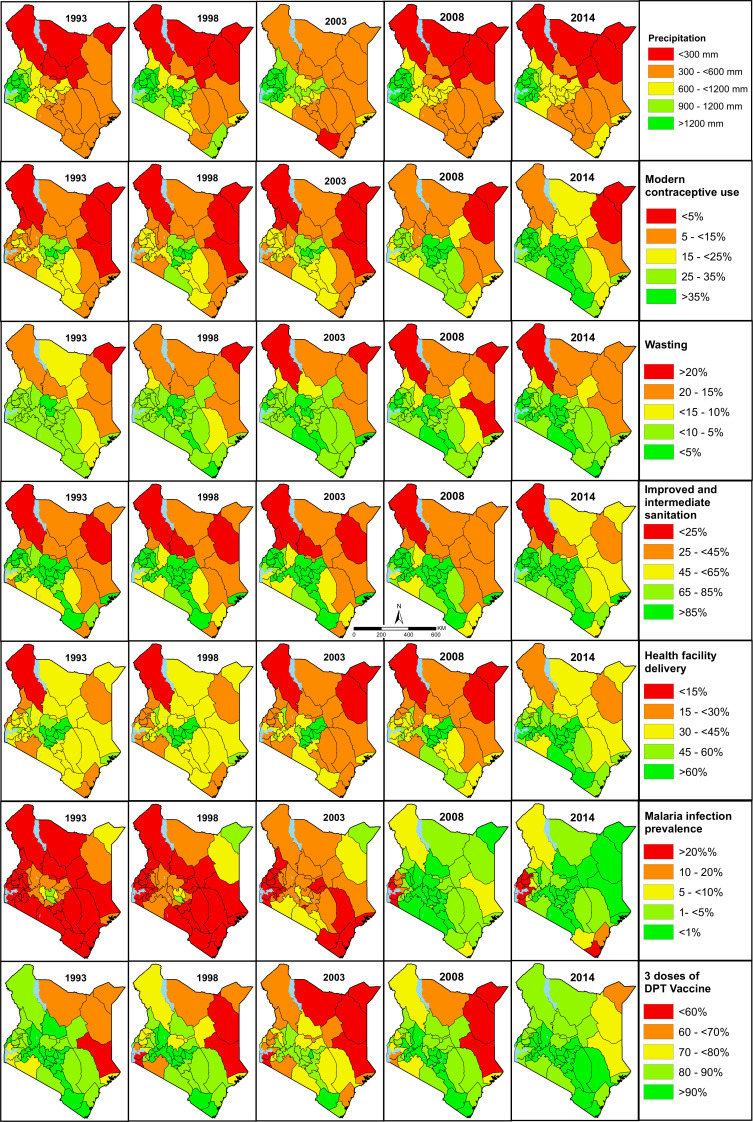
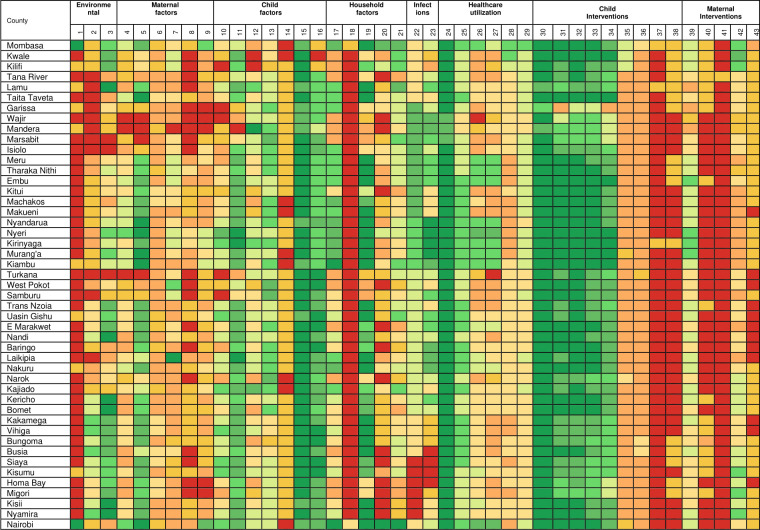
Nationally, the coverage and prevalence were highly variable with 38 factors recording an improvement. The absolute percentage change (1993-2014) was heterogeneous ranging between 1% and 898%. At the county level, the estimates varied across space and over time with a majority showing improvements after 2008 which was preceded by a period of deterioration (late-1990 to early-2000). Counties in Northern Kenya were consistently observed to have lower coverage of interventions and remained disadvantaged in 2014 while areas around Central Kenya had and historically have had higher coverage across all intervention domains. Most factors in Western and South-East Kenya recorded moderate intervention coverage although having a high infection prevalence of both HIV and malaria.
The heterogeneous estimates necessitates prioritisation of the marginalised counties to achieve health equity and improve child survival uniformly across the country. Efforts are required to narrow the gap between counties across all the drivers of child survival. The generated estimates will facilitate improved benchmarking and establish a baseline for monitoring child development goals at subnational level.
为了提高儿童的生存率,有必要描述和理解与儿童生存相关的因素的空间和时间变化,而不仅仅是国家层面的汇总数据,还要以权力下放的卫生规划单位为基础。因此,我们旨在提供与儿童生存相关的因素的国家以下估计数,同时阐明肯尼亚在取得进展、停滞不前和下降的领域。
我们汇集了自 1989 年以来进行的 20 次家庭调查和 3 次人口普查,并将其与 47 个肯尼亚县级行政区的边界进行空间对齐。在 1993 年至 2014 年期间,在县级水平上对 43 个因素进行了贝叶斯时空高斯过程回归模型拟合,这些模型考虑了样本量不足和时空相关性。
在全国范围内,覆盖率和流行率变化很大,有 38 个因素有所改善。绝对百分比变化(1993-2014 年)差异很大,范围在 1%到 898%之间。在县级层面,估计值在空间和时间上存在差异,大多数地区在 2008 年之后都有所改善,而在此之前,情况则有所恶化(1990 年底至 2000 年初)。肯尼亚北部的县一直观察到干预措施的覆盖率较低,并且在 2014 年仍然处于不利地位,而肯尼亚中部地区历来在所有干预领域都有更高的覆盖率。尽管艾滋病毒和疟疾的感染率都很高,但肯尼亚西部和东南部的大多数因素的干预覆盖率适中。
这种异质性的估计需要优先考虑边缘化的县,以实现全国范围内的健康公平,并统一提高儿童的生存率。需要努力缩小所有儿童生存驱动因素的县之间的差距。生成的估计数将有助于改进基准测试,并在国家以下各级建立监测儿童发展目标的基线。