Joseph Noel K, Macharia Peter M, Ouma Paul O, Mumo Jeremiah, Jalang'o Rose, Wagacha Peter W, Achieng Victor O, Ndung'u Eunice, Okoth Peter, Muñiz Maria, Guigoz Yaniss, Panciera Rocco, Ray Nicolas, Okiro Emelda A
Population Health Unit, Kenya Medical Research Institute-Wellcome Trust Research Programme, Nairobi, Kenya.
Health Information System Unit, Ministry of Health, Nairobi, Kenya.
BMC Public Health. 2020 Sep 15;20(1):1407. doi: 10.1186/s12889-020-09486-8.
Poor access to immunisation services remains a major barrier to achieving equity and expanding vaccination coverage in many sub-Saharan African countries. In Kenya, the extent to which spatial access affects immunisation coverage is not well understood. The aim of this study was to quantify spatial accessibility to immunising health facilities and determine its influence on immunisation uptake in Kenya while controlling for potential confounders.
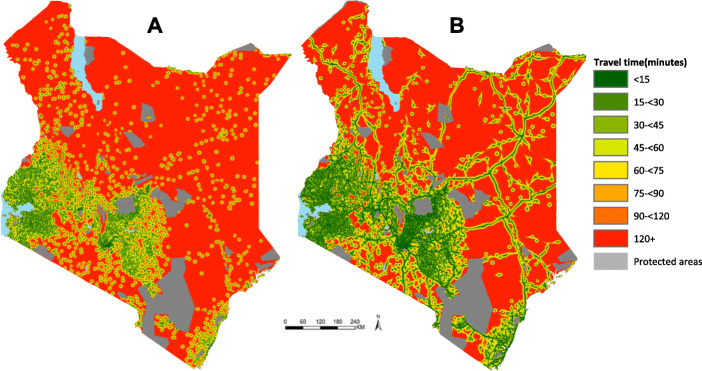
Spatial databases of immunising facilities, road network, land use and elevation were used within a cost friction algorithim to estimate the travel time to immunising health facilities. Two travel scenarios were evaluated; (1) Walking only and (2) Optimistic scenario combining walking and motorized transport. Mean travel time to health facilities and proportions of the total population living within 1-h to the nearest immunising health facility were computed. Data from a nationally representative cross-sectional survey (KDHS 2014), was used to estimate the effect of mean travel time at survey cluster units for both fully immunised status and third dose of diphtheria-tetanus-pertussis (DPT3) vaccine using multi-level logistic regression models.
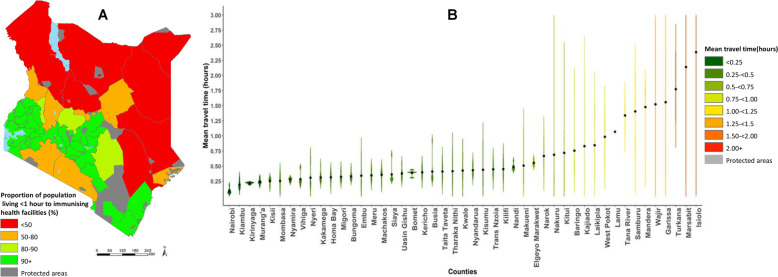
Nationally, the mean travel time to immunising health facilities was 63 and 40 min using the walking and the optimistic travel scenarios respectively. Seventy five percent of the total population were within one-hour of walking to an immunising health facility while 93% were within one-hour considering the optimistic scenario. There were substantial variations across the country with 62%(29/47) and 34%(16/47) of the counties with < 90% of the population within one-hour from an immunising health facility using scenarios 1 and 2 respectively. Travel times > 1-h were significantly associated with low immunisation coverage in the univariate analysis for both fully immunised status and DPT3 vaccine. Children living more than 2-h were significantly less likely to be fully immunised [AOR:0.56(0.33-0.94) and receive DPT3 [AOR:0.51(0.21-0.92) after controlling for household wealth, mother's highest education level, parity and urban/rural residence.
Travel time to immunising health facilities is a barrier to uptake of childhood vaccines in regions with suboptimal accessibility (> 2-h). Strategies that address access barriers in the hardest to reach communities are needed to enhance equitable access to immunisation services in Kenya.
在许多撒哈拉以南非洲国家,获得免疫服务的机会有限仍然是实现公平和扩大疫苗接种覆盖率的主要障碍。在肯尼亚,空间可达性对免疫覆盖率的影响程度尚不清楚。本研究的目的是量化前往提供免疫服务的卫生设施的空间可达性,并在控制潜在混杂因素的同时,确定其对肯尼亚疫苗接种率的影响。
在成本摩擦算法中使用免疫设施、道路网络、土地利用和海拔的空间数据库,以估计前往提供免疫服务的卫生设施的出行时间。评估了两种出行情景;(1)仅步行,(2)步行与机动交通相结合的乐观情景。计算了前往卫生设施的平均出行时间以及居住在距最近的提供免疫服务的卫生设施1小时路程内的总人口比例。使用全国代表性横断面调查(2014年肯尼亚人口与健康调查)的数据,通过多水平逻辑回归模型估计调查聚类单元的平均出行时间对完全免疫状态和白喉-破伤风-百日咳三联疫苗(DPT3)第三剂接种率的影响。
在全国范围内,使用步行和乐观出行情景时,前往提供免疫服务的卫生设施的平均出行时间分别为63分钟和40分钟。75%的总人口步行1小时内可到达提供免疫服务的卫生设施,而考虑乐观情景时这一比例为93%。全国各地存在很大差异,分别有62%(29/47)和34%(16/47)的县,在情景1和情景2下,1小时内可到达提供免疫服务的卫生设施的人口比例低于90%。在完全免疫状态和DPT3疫苗的单变量分析中,出行时间超过1小时与低免疫覆盖率显著相关。在控制家庭财富、母亲的最高教育水平、生育次数和城乡居住情况后,居住超过2小时的儿童完全免疫的可能性显著降低[AOR:0.56(0.33 - 0.94)],接种DPT3的可能性也显著降低[AOR:0.51(0.21 - 0.92)]。
在可达性欠佳(>2小时)的地区,前往提供免疫服务的卫生设施的出行时间是儿童疫苗接种的障碍。需要采取策略解决最难到达社区的获取障碍,以加强肯尼亚免疫服务的公平可及性。