Department of Respiratory Medicine, Nottingham University Hospital NHS Trust, Nottingham NG5 1PB, UK.
Division of Epidemiology and Public Health, School of Medicine, University of Nottingham, Clinical Sciences Building, Nottingham City Hospital Campus, Hucknall Road, Nottingham NG5 1PB, UK.
J Med Microbiol. 2021 Apr;70(4). doi: 10.1099/jmm.0.001350.
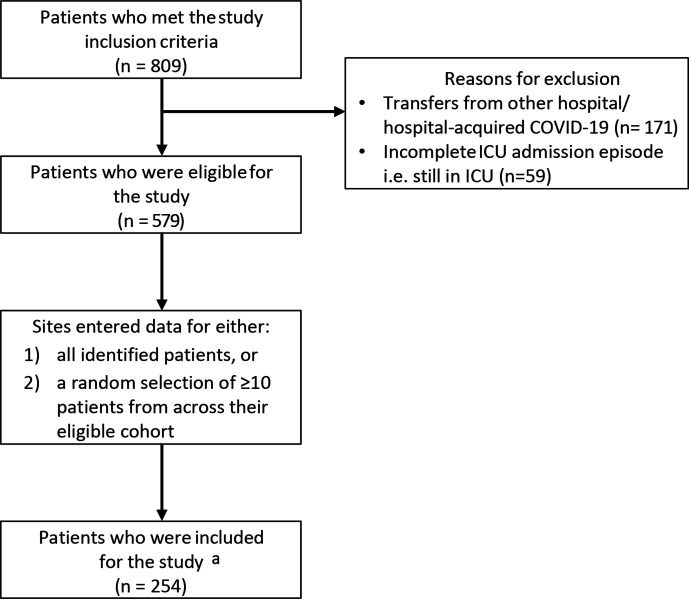
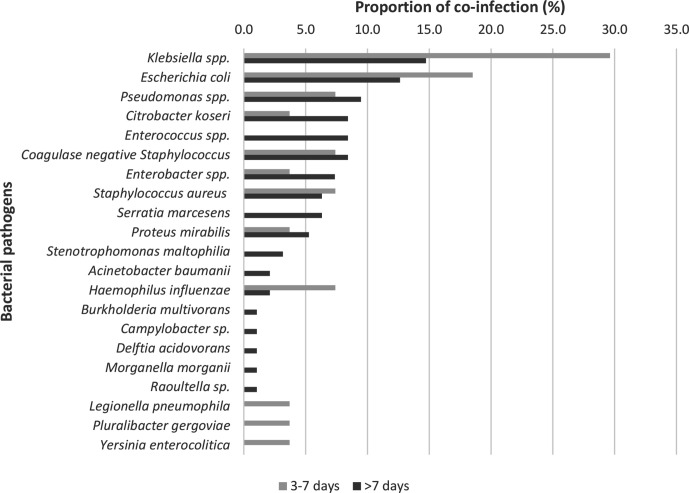
During previous viral pandemics, reported co-infection rates and implicated pathogens have varied. In the 1918 influenza pandemic, a large proportion of severe illness and death was complicated by bacterial co-infection, predominantly and . A better understanding of the incidence of co-infection in patients with COVID-19 infection and the pathogens involved is necessary for effective antimicrobial stewardship. To describe the incidence and nature of co-infection in critically ill adults with COVID-19 infection in England. A retrospective cohort study of adults with COVID-19 admitted to seven intensive care units (ICUs) in England up to 18 May 2020, was performed. Patients with completed ICU stays were included. The proportion and type of organisms were determined at <48 and >48 h following hospital admission, corresponding to community and hospital-acquired co-infections. Of 254 patients studied (median age 59 years (IQR 49-69); 64.6 % male), 139 clinically significant organisms were identified from 83 (32.7 %) patients. Bacterial co-infections/ co-colonisation were identified within 48 h of admission in 14 (5.5 %) patients; the commonest pathogens were (four patients) and (two patients). The proportion of pathogens detected increased with duration of ICU stay, consisting largely of Gram-negative bacteria, particularly and . The co-infection/ co-colonisation rate >48 h after admission was 27/1000 person-days (95 % CI 21.3-34.1). Patients with co-infections/ co-colonisation were more likely to die in ICU (crude OR 1.78,95 % CI 1.03-3.08, =0.04) compared to those without co-infections/ co-colonisation. We found limited evidence for community-acquired bacterial co-infection in hospitalised adults with COVID-19, but a high rate of Gram-negative infection acquired during ICU stay.
在以往的病毒性大流行中,报告的合并感染率和涉及的病原体各不相同。在 1918 年流感大流行中,大量严重疾病和死亡是由细菌合并感染引起的,主要是 和 。为了进行有效的抗菌药物管理,有必要更好地了解 COVID-19 感染患者合并感染的发生率和涉及的病原体。描述英格兰 COVID-19 感染重症成人合并感染的发生率和性质。对截至 2020 年 5 月 18 日在英格兰 7 个重症监护病房(ICU)住院的 COVID-19 成人进行了回顾性队列研究。纳入完成 ICU 住院的患者。在入院后<48 小时和>48 小时,确定了机体的比例和类型,分别对应社区获得性和医院获得性合并感染。在 254 例研究患者中(中位年龄 59 岁(IQR 49-69);64.6%为男性),从 83 例(32.7%)患者中发现了 139 种有临床意义的生物体。14 例(5.5%)患者在入院后 48 小时内发现细菌合并感染/合并定植;最常见的病原体是 (4 例)和 (2 例)。随着 ICU 住院时间的延长,检测到的病原体比例增加,主要是革兰氏阴性菌,特别是 和 。入院后>48 小时的合并感染/合并定植率为 27/1000 人天(95%CI 21.3-34.1)。与无合并感染/合并定植的患者相比,合并感染/合并定植的患者 ICU 死亡率更高(粗 OR 1.78,95%CI 1.03-3.08,=0.04)。我们发现,在 COVID-19 住院成人中,社区获得性细菌性合并感染的证据有限,但 ICU 住院期间获得的革兰氏阴性感染率很高。