Grinda Thomas, Joyon Natacha, Lusque Amélie, Lefèvre Sarah, Arnould Laurent, Penault-Llorca Frédérique, Macgrogan Gaëtan, Treilleux Isabelle, Vincent-Salomon Anne, Haudebourg Juliette, Maran-Gonzalez Aurélie, Charafe-Jauffret Emmanuelle, Courtinard Coralie, Franchet Camille, Verriele Véronique, Brain Etienne, Tas Patrick, Blanc-Fournier Cécile, Leroux Agnès, Loussouarn Delphine, Berghian Anca, Brabencova Eva, Ghnassia Jean Pierre, Scoazec Jean-Yves, Delaloge Suzette, Filleron Thomas, Lacroix-Triki Magali
Gustave Roussy Cancer Campus, Villejuif, France.
Institut Claudius Regaud, IUCT-Oncopôle, Toulouse, France.
NPJ Breast Cancer. 2021 Apr 16;7(1):41. doi: 10.1038/s41523-021-00252-6.
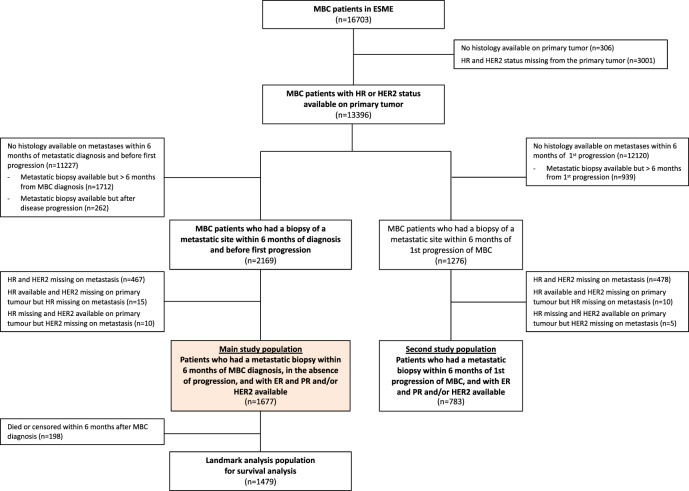
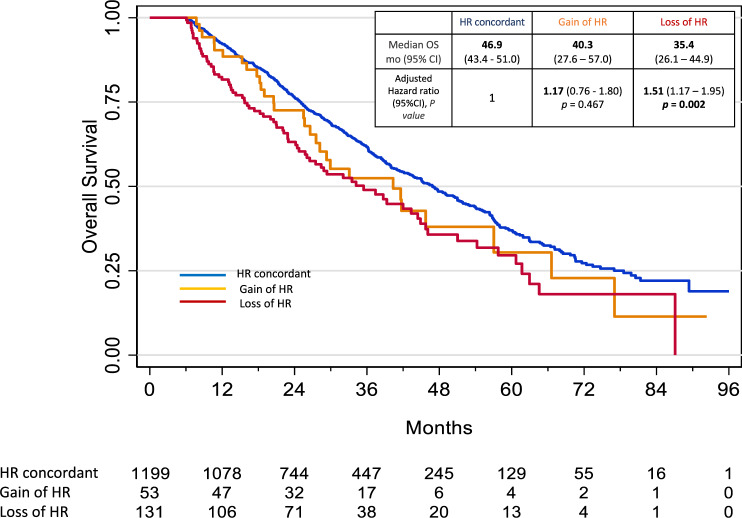
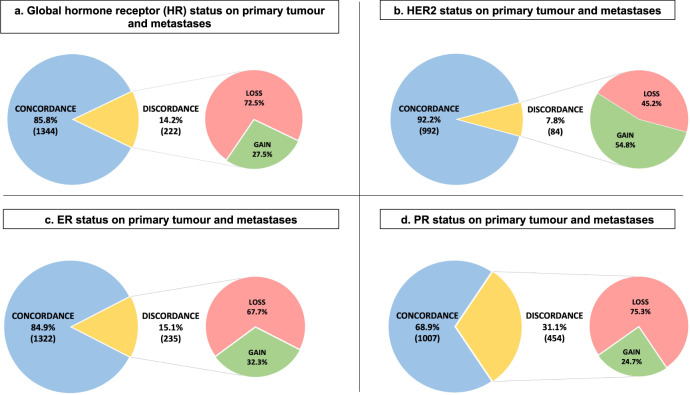
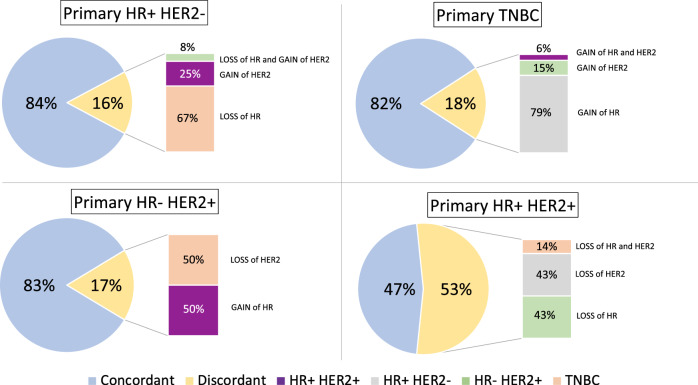
Expression of hormone receptor (HR) for estrogens (ER) and progesterone (PR) and HER2 remains the cornerstone to define the therapeutic strategy for breast cancer patients. We aimed to compare phenotypic profiles between matched primary and metastatic breast cancer (MBC) in the ESME database, a National real-life multicenter cohort of MBC patients. Patients with results available on both primary tumour and metastatic disease within 6 months of MBC diagnosis and before any tumour progression were eligible for the main analysis. Among the 16,703 patients included in the database, 1677 (10.0%) had available biopsy results at MBC diagnosis and on matched primary tumour. The change rate of either HR or HER2 was 27.0%. Global HR status changed (from positive = either ER or PR positive, to negative = both negative; and reverse) in 14.2% of the cases (expression loss in 72.5% and gain in 27.5%). HER2 status changed in 7.8% (amplification loss in 45.2%). The discordance rate appeared similar across different biopsy sites. Metastasis to bone, HER2+ and RH+/HER2- subtypes and previous adjuvant endocrine therapy, but not relapse interval were associated with an HR discordance in multivariable analysis. Loss of HR status was significantly associated with a risk of death (HR adjusted = 1.51, p = 0.002) while gain of HR and HER2 discordance was not. In conclusion, discordance of HR and HER2 expression between primary and metastatic breast cancer cannot be neglected. In addition, HR loss is associated with worse survival. Sampling metastatic sites is essential for treatment adjustment.
雌激素(ER)和孕激素(PR)的激素受体(HR)以及HER2的表达仍然是确定乳腺癌患者治疗策略的基石。我们旨在比较ESME数据库中配对的原发性和转移性乳腺癌(MBC)之间的表型特征,该数据库是一个全国性的MBC患者真实多中心队列。在MBC诊断后6个月内且在任何肿瘤进展之前,原发性肿瘤和转移性疾病均有可用结果的患者符合主要分析标准。在数据库纳入的16703例患者中,1677例(10.0%)在MBC诊断时及配对的原发性肿瘤有可用的活检结果。HR或HER2的变化率为27.0%。整体HR状态改变(从阳性=ER或PR阳性,变为阴性=两者均阴性;反之亦然)的病例占14.2%(表达缺失占72.5%,增加占27.5%)。HER2状态改变的占7.8%(扩增缺失占45.2%)。不同活检部位的不一致率似乎相似。多变量分析显示,骨转移、HER2阳性和HR阳性/HER2阴性亚型以及既往辅助内分泌治疗,但不包括复发间隔,与HR不一致相关。HR状态缺失与死亡风险显著相关(校正后HR=1.51,p=0.002),而HR增加和HER2不一致则无此关联。总之,原发性和转移性乳腺癌之间HR和HER2表达的不一致不容忽视。此外,HR缺失与较差的生存率相关。对转移部位进行采样对于治疗调整至关重要。