Chidambaran Vidya, Pilipenko Valentina, Jegga Anil G, Geisler Kristie, Martin Lisa J
Department of Anesthesiology, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States.
Division of Human Genetics, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States.
Front Genet. 2021 Mar 23;12:594250. doi: 10.3389/fgene.2021.594250. eCollection 2021.
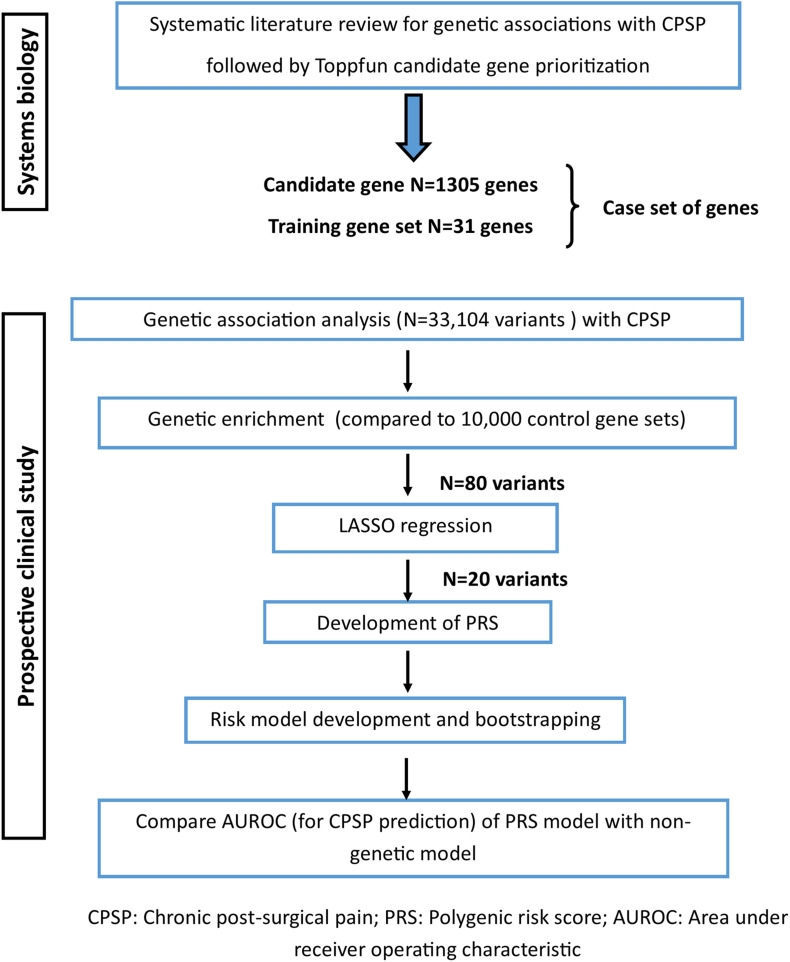
Incorporation of genetic factors in psychosocial/perioperative models for predicting chronic postsurgical pain (CPSP) is key for personalization of analgesia. However, single variant associations with CPSP have small effect sizes, making polygenic risk assessment important. Unfortunately, pediatric CPSP studies are not sufficiently powered for unbiased genome wide association (GWAS). We previously leveraged systems biology to identify candidate genes associated with CPSP. The goal of this study was to use systems biology prioritized gene enrichment to generate polygenic risk scores (PRS) for improved prediction of CPSP in a prospectively enrolled clinical cohort.
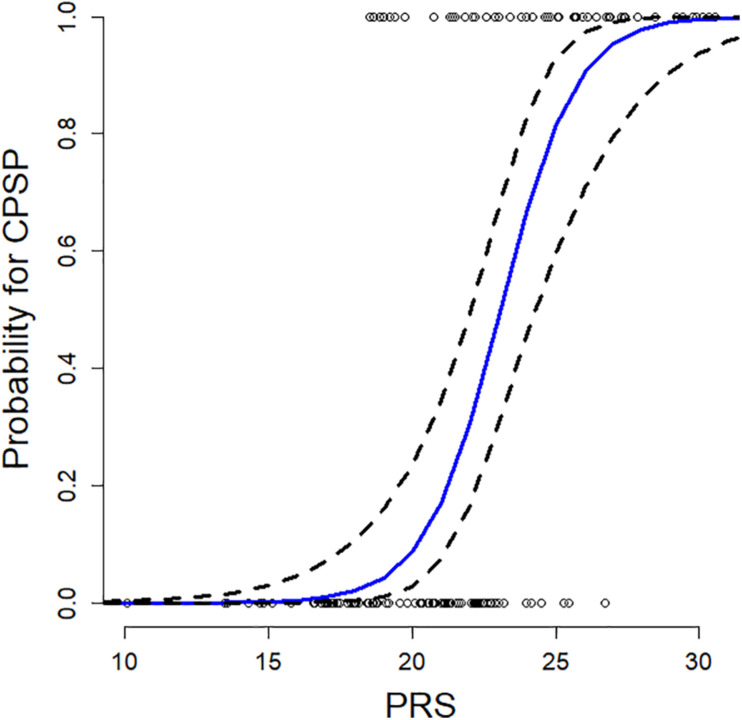
In a prospectively recruited cohort of 171 adolescents (14.5 ± 1.8 years, 75.4% female) undergoing spine fusion, we collected data about anesthesia/surgical factors, childhood anxiety sensitivity (CASI), acute pain/opioid use, pain outcomes 6-12 months post-surgery and blood (for DNA extraction/genotyping). We previously prioritized candidate genes using computational approaches based on similarity for functional annotations with a literature-derived "training set." In this study, we tested ranked deciles of 1336 prioritized genes for increased representation of variants associated with CPSP, compared to 10,000 randomly selected control sets. Penalized regression (LASSO) was used to select final variants from enriched variant sets for calculation of PRS. PRS incorporated regression models were compared with previously published non-genetic models for predictive accuracy.
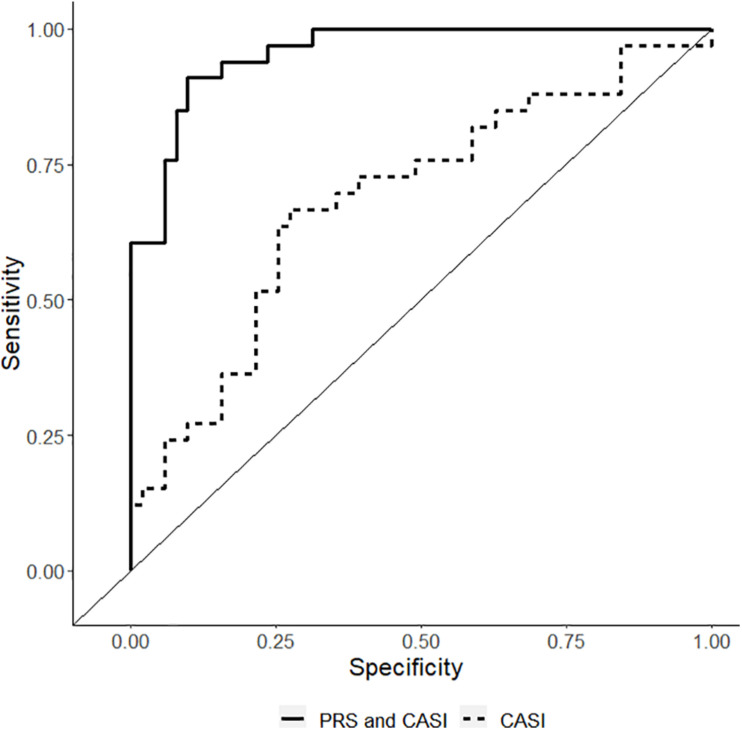
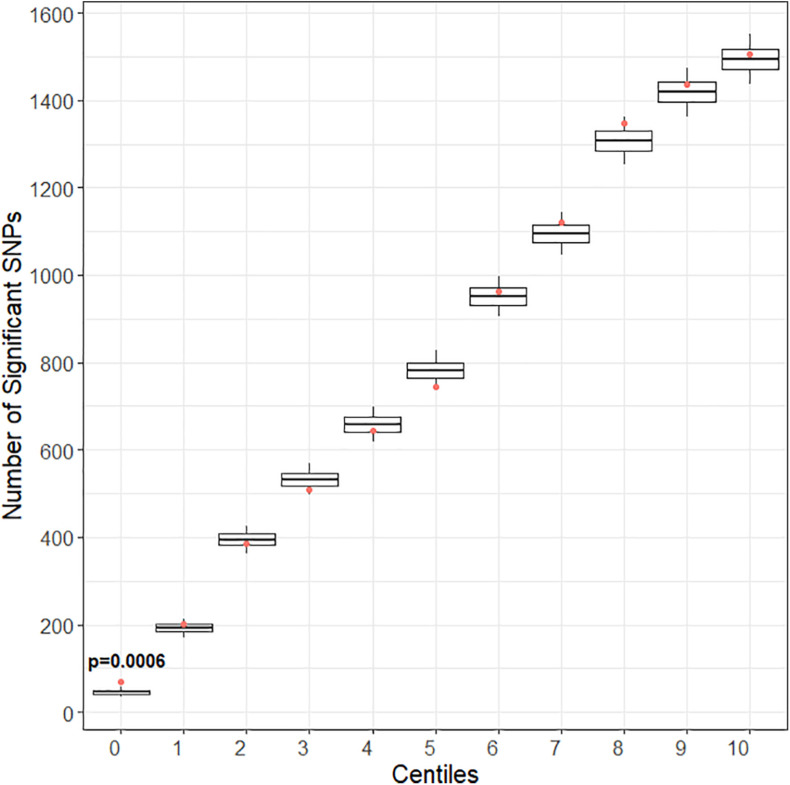
Incidence of CPSP in the prospective cohort was 40.4%. 33,104 case and 252,590 control variants were included for association analyses. The smallest gene set enriched for CPSP had 80/1010 variants associated with CPSP ( < 0.05), significantly higher than in 10,000 randomly selected control sets ( = 0.0004). LASSO selected 20 variants for calculating weighted PRS. Model adjusted for covariates including PRS had AUROC of 0.96 (95% CI: 0.92-0.99) for CPSP prediction, compared to 0.70 (95% CI: 0.59-0.82) for non-genetic model ( < 0.001). Odds ratios and positive regression coefficients for the final model were internally validated using bootstrapping: PRS [OR 1.98 (95% CI: 1.21-3.22); β 0.68 (95% CI: 0.19-0.74)] and CASI [OR 1.33 (95% CI: 1.03-1.72); β 0.29 (0.03-0.38)].
Systems biology guided PRS improved predictive accuracy of CPSP risk in a pediatric cohort. They have potential to serve as biomarkers to guide risk stratification and tailored prevention. Findings highlight systems biology approaches for deriving PRS for phenotypes in cohorts less amenable to large scale GWAS.
将遗传因素纳入心理社会/围手术期模型以预测慢性术后疼痛(CPSP)是实现镇痛个性化的关键。然而,单基因变异与CPSP的关联效应量较小,使得多基因风险评估变得重要。不幸的是,儿科CPSP研究的样本量不足以进行无偏倚的全基因组关联研究(GWAS)。我们之前利用系统生物学来识别与CPSP相关的候选基因。本研究的目的是使用系统生物学优先排序的基因富集来生成多基因风险评分(PRS),以改善对前瞻性纳入的临床队列中CPSP的预测。
在一个前瞻性招募的171名接受脊柱融合手术的青少年队列(14.5±1.8岁,75.4%为女性)中,我们收集了关于麻醉/手术因素、儿童焦虑敏感性(CASI)、急性疼痛/阿片类药物使用、术后6 - 12个月的疼痛结局以及血液(用于DNA提取/基因分型)的数据。我们之前基于与文献衍生的“训练集”功能注释的相似性,使用计算方法对候选基因进行了优先排序。在本研究中,与10000个随机选择的对照组相比,我们测试了1336个优先排序基因的十分位数,以确定与CPSP相关变异的代表性增加情况。使用惩罚回归(LASSO)从富集的变异集中选择最终变异以计算PRS。将纳入PRS的回归模型与之前发表的非遗传模型的预测准确性进行比较。
前瞻性队列中CPSP的发生率为40.4%。纳入33104个病例变异和252590个对照变异进行关联分析。富集CPSP的最小基因集有80/1010个变异与CPSP相关(<0.05),显著高于10000个随机选择的对照组(=0.0004)。LASSO选择了20个变异来计算加权PRS。调整包括PRS在内的协变量后的模型对CPSP预测的曲线下面积(AUROC)为0.96(95%CI:0.92 - 0.99),而非遗传模型的AUROC为0.70(95%CI:0.59 - 0.82)(<0.001)。最终模型的优势比和正回归系数通过自抽样进行内部验证:PRS [优势比1.98(95%CI:1.21 - 3.22);β0.68(95%CI:0.19 - 0.74)]和CASI [优势比1.33(95%CI:1.03 - 1.72);β0.29(0.03 - 0.38)]。
系统生物学指导的PRS提高了儿科队列中CPSP风险的预测准确性。它们有潜力作为生物标志物来指导风险分层和个性化预防。研究结果突出了系统生物学方法在难以进行大规模GWAS的队列中推导表型PRS的应用。