Delitto Anthony, Patterson Charity G, Stevans Joel M, Freburger Janet K, Khoja Samannaaz S, Schneider Michael J, Greco Carol M, Freel Jennifer A, Sowa Gwendolyn A, Wasan Ajay D, Brennan Gerard P, Hunter Stephen J, Minick Kate I, Wegener Stephen T, Ephraim Patti L, Beneciuk Jason M, George Steven Z, Saper Robert B
School of Health and Rehabilitation Sciences, University of Pittsburgh, 4029 Forbes Tower, Pittsburgh, PA 15260 USA.
School of Health and Rehabilitation Sciences, University of Pittsburgh, 100 Technology Drive, Pittsburgh, PA 15219 USA.
EClinicalMedicine. 2021 Mar 30;34:100795. doi: 10.1016/j.eclinm.2021.100795. eCollection 2021 Apr.
Many patients with acute low back pain (LBP) first seek care from primary care physicians. Evidence is lacking for interventions to prevent transition to chronic LBP in this setting. We aimed to test if implementation of a risk-stratified approach to care would result in lower rates of chronic LBP and improved self-reported disability.
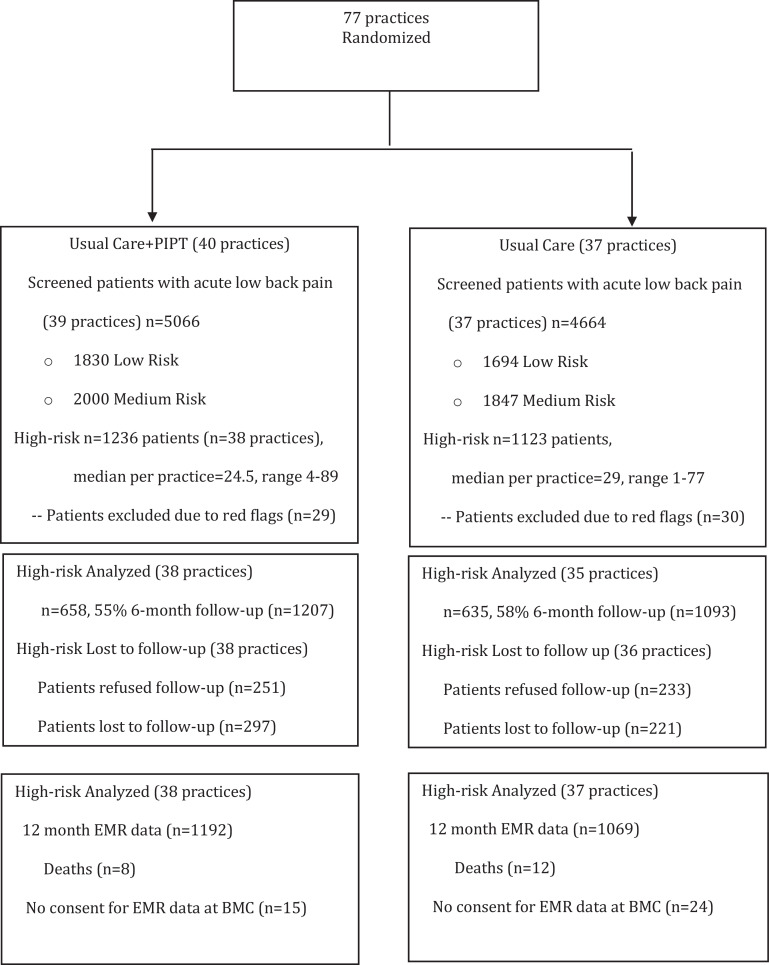
We conducted a pragmatic, cluster randomized trial using 77 primary care clinics in four health care systems across the United States. Practices were randomly assigned to a stratified approach to care (intervention) or usual care (control). Using the STarTBack screening tool, adults with acute LBP were screened low, medium, and high-risk. Patients screened as high-risk were eligible. The intervention included electronic best practice alerts triggering referrals for psychologically informed physical therapy (PIPT). PIPT education was targeted to community clinics geographically close to intervention primary care clinics. Primary outcomes were transition to chronic LBP and self-reported disability at six months. Trial Registry: ClinicalTrials.gov NCT02647658.
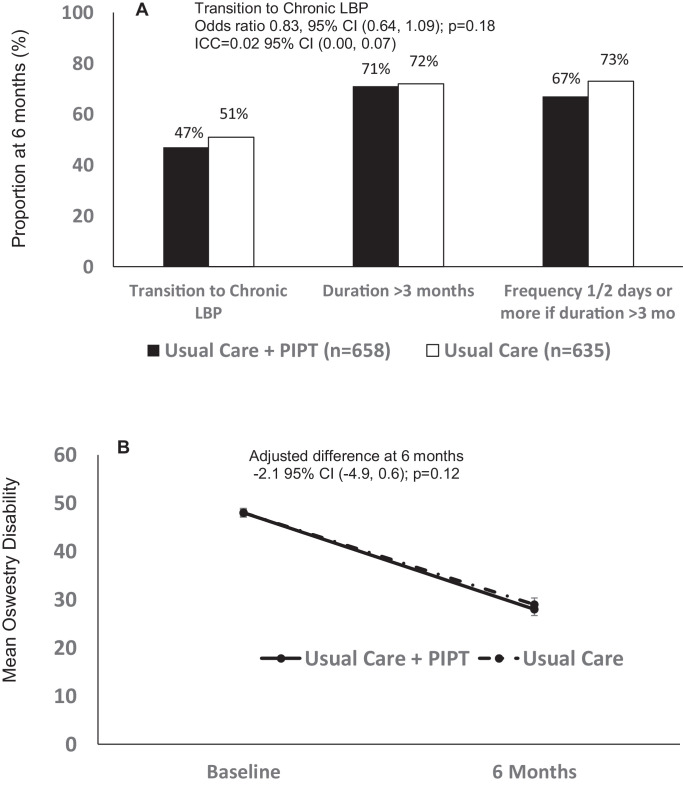
Between May 2016 and June 2018, 1207 patients from 38 intervention and 1093 from 37 control practices were followed. In the intervention arm, around 50% of patients were referred for physical therapy (36% for PIPT) compared to 30% in the control. At 6 months, 47% of patients reported transition to chronic LBP in the intervention arm (38 practices, = 658) versus 51% of patients in the control arm (35 practices, = 635; OR=0.83 95% CI 0.64, 1.09; = 0.18). No differences in disability were detected (difference -2·1, 95% CI -4.9-0.6; = 0.12). Opioids and imaging were prescribed in 22%-25% and 23%-26% of initial visits, for intervention and control, respectively. Twelve-month LBP utilization was similar in the two groups.
There were no differences detected in transition to chronic LBP among patients presenting with acute LBP using a stratified approach to care. Opioid and imaging prescribing rates were non-concordant with clinical guidelines.
Patient-Centered Outcomes Research Institute (PCORI) contract # PCS-1402-10867.
许多急性腰痛(LBP)患者首先会寻求初级保健医生的治疗。在这种情况下,缺乏预防转变为慢性腰痛的干预措施的证据。我们旨在测试实施风险分层护理方法是否会降低慢性腰痛的发生率并改善自我报告的残疾状况。
我们在美国四个医疗系统中的77家初级保健诊所进行了一项实用的整群随机试验。这些诊所被随机分配到分层护理方法(干预组)或常规护理(对照组)。使用STarTBack筛查工具,将患有急性腰痛的成年人筛查为低、中、高风险。筛查为高风险的患者符合条件。干预措施包括电子最佳实践警报,触发转介至心理知情物理治疗(PIPT)。PIPT教育针对地理位置靠近干预初级保健诊所的社区诊所。主要结局是六个月时转变为慢性腰痛和自我报告的残疾状况。试验注册:ClinicalTrials.gov NCT02647658。
在2016年5月至2018年6月期间,对来自38个干预诊所的1207名患者和来自37个对照诊所的1093名患者进行了随访。在干预组中,约50%的患者被转介接受物理治疗(36%接受PIPT),而对照组为30%。在6个月时,干预组中有47%的患者报告转变为慢性腰痛(38个诊所,n = 658),而对照组为51%(35个诊所,n = 635;OR = 0.83,95% CI 0.64,1.09;P = 0.18)。未检测到残疾方面的差异(差异为-2·1,95% CI -4.9 - 0.6;P = 0.12)。干预组和对照组分别有22% - 25%和23% - 26%的初次就诊患者开具了阿片类药物和进行了影像学检查。两组在12个月时的腰痛治疗利用率相似。
使用分层护理方法对急性腰痛患者进行治疗,在转变为慢性腰痛方面未检测到差异。阿片类药物和影像学检查的处方率与临床指南不一致。
以患者为中心的结果研究机构(PCORI)合同编号PCS - 1402 - 10867。