Mayo Clinic Heath System, Eau Claire, Wisconsin, USA.
University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA.
United European Gastroenterol J. 2021 Mar;9(2):139-149. doi: 10.1002/ueg2.12057.
Persistent organ failure (POF) is the strongest determinant of mortality in acute pancreatitis (AP). There is a paucity of data regarding the impact of different POF attributes on mortality and the role of different characteristics of systemic inflammatory response syndrome (SIRS) in the risk of developing POF.
We aimed to assess the association of POF dynamic features with mortality and SIRS characteristics with POF.
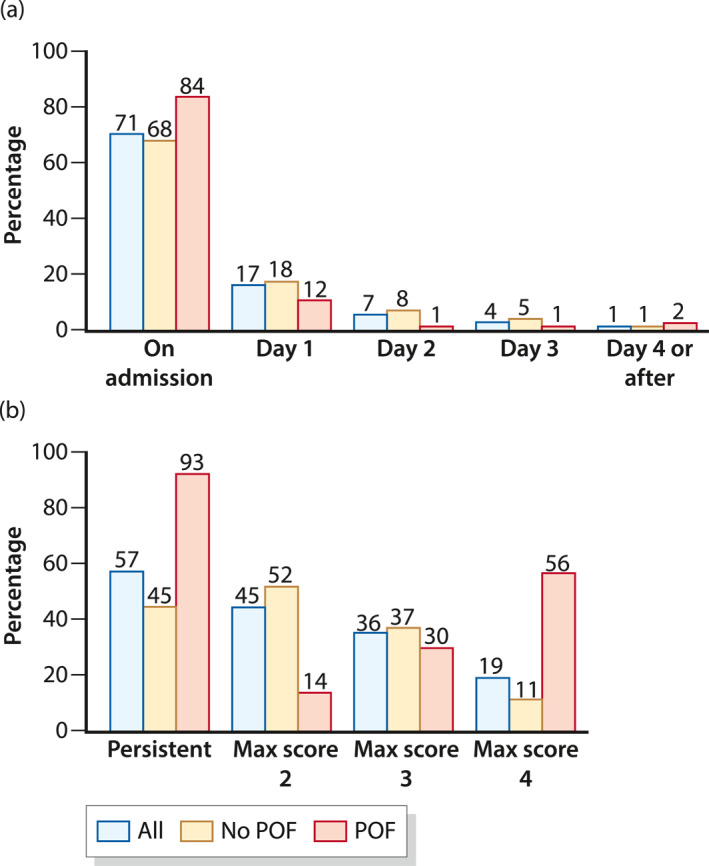
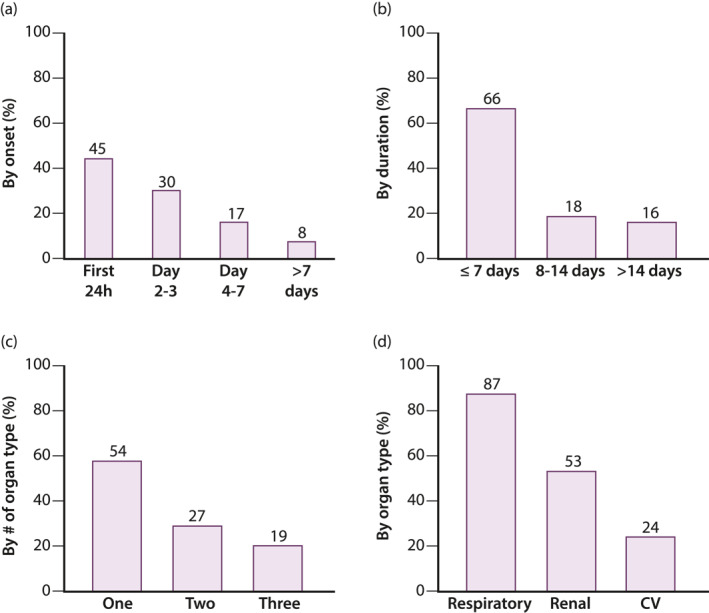
We studied 1544 AP subjects prospectively enrolled at 22 international centers (APPRENTICE consortium). First, we estimated the association of onset, duration, and maximal score of SIRS with POF. Then, we evaluated the risk of mortality based on POF onset, duration, number, type, and sequence of organs affected. Analyses were adjusted for potential confounders.
58% had SIRS, 11% developed POF, and 2.5% died. Early SIRS, persistent SIRS, and maximal SIRS score ≥ 3 were independently associated with higher risk of POF (p < 0.05). Mortality risk in POF was higher with two (33%, odds ratio [OR] = 10.8, 3.3-34.9) and three (48%, OR = 20.2, 5.9-68.6) organs failing, in comparison to single POF (4%). In subjects with multiple POF, mortality was higher when the cardiovascular and respiratory systems failed first or concurrently as compared to when the renal system failed first or concurrently with other organ (p < 0.05). In multivariate regression model, the number and sequence of organs affected in POF were associated with mortality (p < 0.05). Onset and duration of POF had no impact mortality.
In AP patients with POF, the risk of mortality is influenced by the number, type, and sequence of organs affected. These results are useful for future revisions of AP severity classification systems.
持续性器官衰竭(POF)是急性胰腺炎(AP)患者死亡的最强决定因素。关于不同 POF 特征对死亡率的影响以及全身炎症反应综合征(SIRS)不同特征在发生 POF 风险中的作用的数据很少。
我们旨在评估 POF 动态特征与死亡率以及 SIRS 特征与 POF 的关系。
我们前瞻性地研究了 22 个国际中心(APPRENTICE 联盟)纳入的 1544 名 AP 患者。首先,我们估计 SIRS 的起始时间、持续时间和最大评分与 POF 的关系。然后,我们根据 POF 的起始时间、持续时间、累及器官的数量、类型和顺序评估死亡率的风险。分析调整了潜在的混杂因素。
58%的患者有 SIRS,11%发生 POF,2.5%死亡。早期 SIRS、持续性 SIRS 和最大 SIRS 评分≥3 与 POF 的高风险独立相关(p<0.05)。与单一 POF(4%)相比,有两个(33%,OR=10.8,3.3-34.9)和三个(48%,OR=20.2,5.9-68.6)器官衰竭的 POF 患者死亡率更高。在有多个 POF 的患者中,当心血管和呼吸系统首先衰竭或同时衰竭,与当肾脏系统首先衰竭或与其他器官同时衰竭相比,死亡率更高(p<0.05)。在多变量回归模型中,POF 累及器官的数量和顺序与死亡率相关(p<0.05)。POF 的起始时间和持续时间对死亡率没有影响。
在 POF 的 AP 患者中,死亡率的风险受受累器官的数量、类型和顺序的影响。这些结果对未来的 AP 严重程度分类系统修订有用。