Department of Anesthesia, Critical Care and Pain Medicine, Beth Israel Deaconess Medical Center, 330 Brookline Ave, Boston, MA, 02215, USA.
BMC Anesthesiol. 2021 Apr 19;21(1):120. doi: 10.1186/s12871-021-01332-7.
In this study, we explored the utility of intravenous opioid rescue analgesia in the post anesthesia care unit (PACU-OpResc) as a single marker of thoracic epidural analgesia (TEA) failure and evaluated the resource implications and quality improvement applications of this measure.
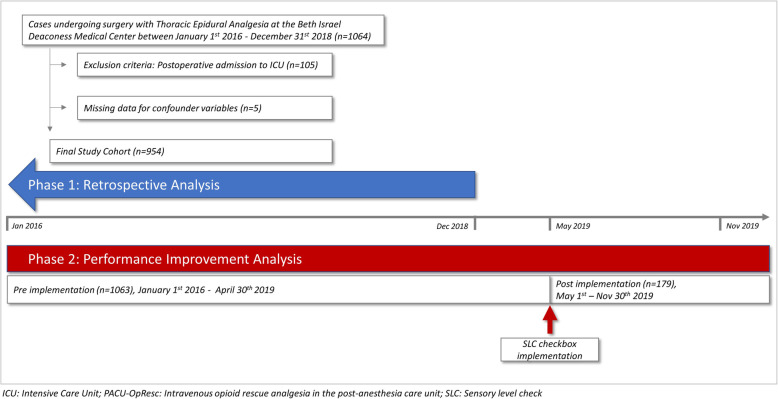
We performed a retrospective analysis of all TEA placements over a three-year period at a single academic medical center in Boston, Massachusetts. The study exposure was PACU-OpResc. Primary outcome was PACU length of stay (LOS). Secondary outcomes included reasons for delayed PACU discharge and intraoperative hypotension. The analyses were adjusted for confounding variables including patient comorbidities, surgical complexity, intraoperative intravenous opioids, chronic opioid use and local anesthetic bolus through TEA catheter. Post analysis chart review was conducted to determine the positive predictive value (PPV) of PACU-OpResc for inadequate TEA. As a first Plan-Do-Study-Act cycle, we then introduced a checkbox for documentation of a sensory level check after TEA placement. Post implementation data was collected for 7 months.
PACU-OpResc was required by 211 (22.1%) patients who received preoperative TEA, was associated with longer PACU LOS (incidence rate ratio 1.20, 95% CI:1.07-1.34, p = 0.001) and delayed discharge due to inadequate pain control (odds ratio 5.15, 95% CI 3.51-7.57, p < 0.001). PACU-OpResc had a PPV of 76.3 and 60.4% for re-evaluation and manipulation of the TEA catheter in PACU, respectively. Following implementation of a checkbox, average monthly compliance with documented sensory level check after TEA placement was noted to be 39.7%. During this time, a reduction of 8.2% in the rate of PACU-OpResc was observed.
This study demonstrates that PACU-OpResc can be used as a quality assurance measure or surrogate for TEA efficacy, to track performance and monitor innovation efforts aimed at improving analgesia, such as our intervention to facilitate sensory level checks and reduced PACU-OpResc.
not applicable.
在这项研究中,我们探讨了静脉内阿片类药物解救镇痛在麻醉后恢复室(PACU-OpResc)中的效用,将其作为胸段硬膜外镇痛(TEA)失败的单一标志物,并评估了该措施的资源影响和质量改进应用。
我们对马萨诸塞州波士顿一家学术医疗中心三年内所有 TEA 放置的患者进行了回顾性分析。研究暴露于 PACU-OpResc。主要结局为 PACU 住院时间(LOS)。次要结局包括 PACU 延迟出院的原因和术中低血压。通过 TEA 导管中的患者合并症、手术复杂性、术中静脉内阿片类药物、慢性阿片类药物使用和局部麻醉剂推注对分析进行了混杂变量调整。术后进行图表审查以确定 PACU-OpResc 对 TEA 不足的阳性预测值(PPV)。作为第一个计划-执行-研究-行动(Plan-Do-Study-Act)循环,我们引入了一个用于记录 TEA 放置后感觉水平检查的复选框。实施后收集了 7 个月的数据。
211 名(22.1%)接受术前 TEA 的患者需要 PACU-OpResc,这与 PACU LOS 延长(发生率比 1.20,95%CI:1.07-1.34,p=0.001)和因疼痛控制不足导致延迟出院有关(优势比 5.15,95%CI 3.51-7.57,p<0.001)。PACU-OpResc 在 PACU 中重新评估和处理 TEA 导管的 PPV 分别为 76.3%和 60.4%。实施复选框后,平均每月记录 TEA 放置后感觉水平检查的依从性为 39.7%。在此期间,PACU-OpResc 的发生率降低了 8.2%。
这项研究表明,PACU-OpResc 可作为 TEA 疗效的质量保证措施或替代指标,用于跟踪绩效和监测旨在改善镇痛的创新努力,例如我们的干预措施以促进感觉水平检查和减少 PACU-OpResc。
不适用。