Section of Preventive Medicine Department of Medicine Boston University School of Medicine Boston MA.
Section of Cardiology Department of Medicine Boston University School of Medicine Boston MA.
J Am Heart Assoc. 2021 May 4;10(9):e016524. doi: 10.1161/JAHA.120.016524. Epub 2021 Apr 21.
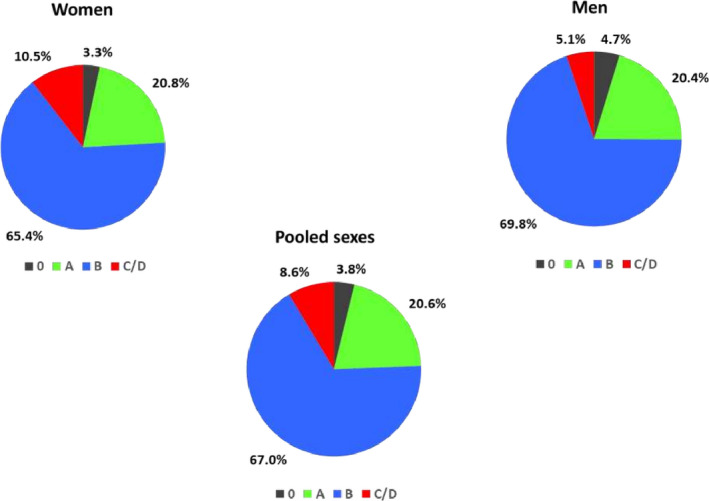
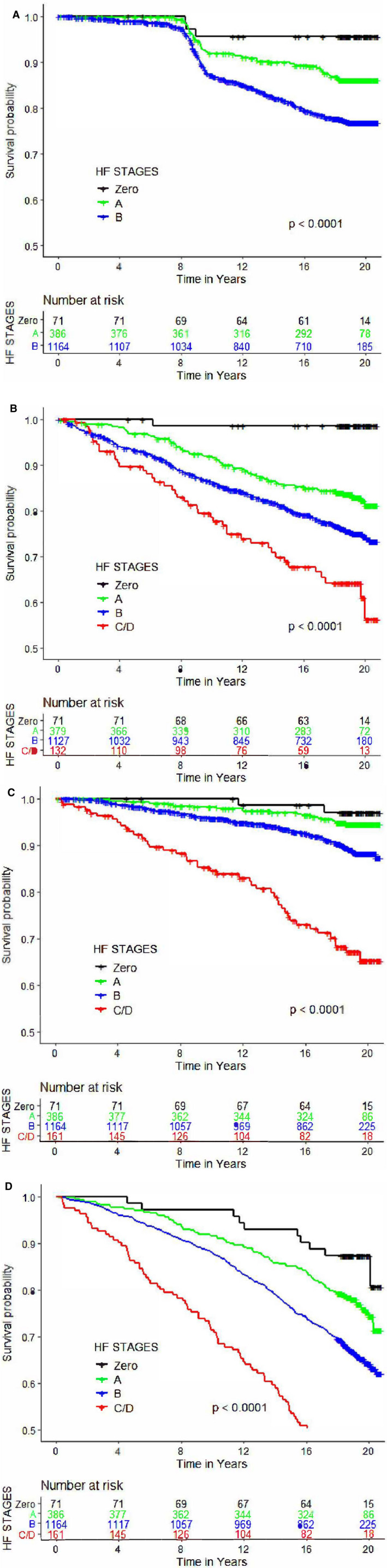
Background Black individuals have a higher burden of risk factors for heart failure (HF) and subclinical left ventricular remodeling. Methods and Results We evaluated 1871 Black participants in the Atherosclerosis Risk in Communities Study cohort who attended a routine examination (1993-1996, median age 58 years) when they underwent echocardiography. We estimated the prevalences of 4 HF stages: (1) : no risk factors; (2) : presence of HF risk factors (hypertension, diabetes mellitus, obesity, smoking, dyslipidemia, coronary artery disease without clinical myocardial infarction), no cardiac structural/functional abnormality; (3) : presence of prior myocardial infarction, systolic dysfunction, left ventricular hypertrophy, regional wall motion abnormality, or left ventricular enlargement; and (4) : prevalent HF. We assessed the incidence of clinical HF, atherosclerotic cardiovascular disease events, and all-cause mortality on follow-up according to HF stage. The prevalence of HF Stages 0, A, B, and C/D were 3.8%, 20.6%, 67.0%, and 8.6%, respectively, at baseline. On follow-up (median 19.0 years), 309 participants developed overt HF, 390 incurred new-onset cardiovascular disease events, and 651 individuals died. Incidence rates per 1000 person-years for overt HF, cardiovascular disease events, and death, respectively, were Stage 0, 2.4, 0.8, and 7.6; Stage A, 7.4, 9.7, and 13.5; Stage B 13.6, 15.9, and 22.0. Stage B HF was associated with a 1.5- to 2-fold increased adjusted risk of HF, cardiovascular disease events and death compared with Stages 0/A. Conclusions In our large community-based sample of Black individuals, we observed a strikingly high prevalence of Stage B HF in middle age that was a marker of high cardiovascular morbidity and mortality.
黑人个体患心力衰竭(HF)和亚临床左心室重构的风险因素负担更高。
我们评估了参加动脉粥样硬化风险社区研究队列的 1871 名黑人参与者,他们在常规检查时(1993-1996 年,中位年龄 58 岁)接受了超声心动图检查。我们估计了 4 个 HF 阶段的患病率:(1):无风险因素;(2):存在 HF 风险因素(高血压、糖尿病、肥胖、吸烟、血脂异常、无临床心肌梗死的冠状动脉疾病),无心脏结构/功能异常;(3):存在先前的心肌梗死、收缩功能障碍、左心室肥厚、局部壁运动异常或左心室扩大;(4):HF 流行。根据 HF 阶段,我们评估了随访期间临床 HF、动脉粥样硬化性心血管疾病事件和全因死亡率的发生率。HF 阶段 0、A、B 和 C/D 的基线患病率分别为 3.8%、20.6%、67.0%和 8.6%。在随访期间(中位数 19.0 年),309 名参与者出现明显 HF,390 名参与者发生新发心血管疾病事件,651 名参与者死亡。每 1000 人年的明显 HF、心血管疾病事件和死亡率发生率分别为阶段 0:2.4、9.7 和 13.5;阶段 B:13.6、15.9 和 22.0。与阶段 0/A 相比,HF 阶段 B 的 HF、心血管疾病事件和死亡的调整风险增加了 1.5-2 倍。
在我们的大型黑人社区样本中,我们观察到中年 HF 阶段 B 的患病率非常高,这是心血管发病率和死亡率高的标志。