Holzknecht Magdalena, Reindl Martin, Tiller Christina, Reinstadler Sebastian J, Lechner Ivan, Pamminger Mathias, Schwaiger Johannes P, Klug Gert, Bauer Axel, Metzler Bernhard, Mayr Agnes
University Clinic of Internal Medicine III, Cardiology and Angiology, Medical University of Innsbruck, Anichstrasse 35, 6020, Innsbruck, Austria.
University Clinic of Radiology, Medical University of Innsbruck, Anichstrasse 35, 6020, Innsbruck, Austria.
Clin Res Cardiol. 2021 Oct;110(10):1599-1611. doi: 10.1007/s00392-021-01855-6. Epub 2021 Apr 21.
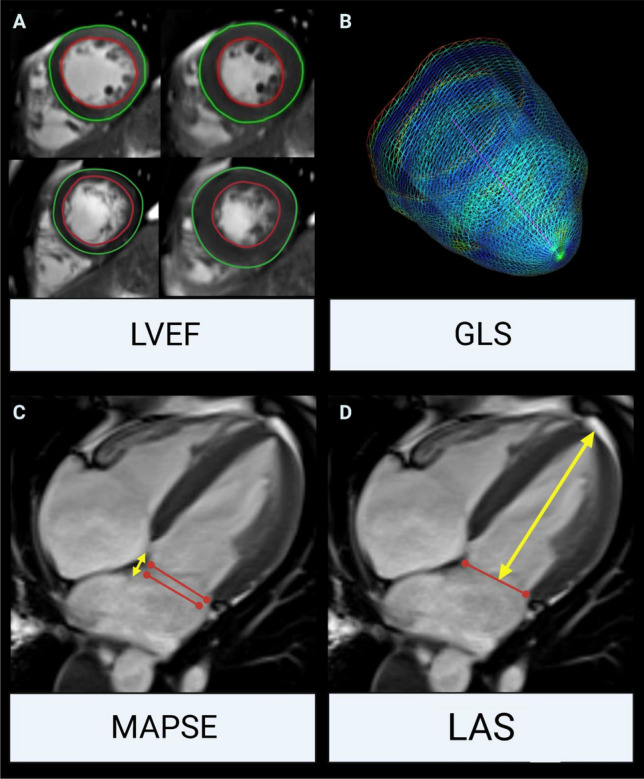
We aimed to investigate the comparative prognostic value of left ventricular ejection fraction (LVEF), mitral annular plane systolic excursion (MAPSE), fast manual long-axis strain (LAS) and global longitudinal strain (GLS) determined by cardiac magnetic resonance (CMR) in patients after ST-segment elevation myocardial infarction (STEMI).
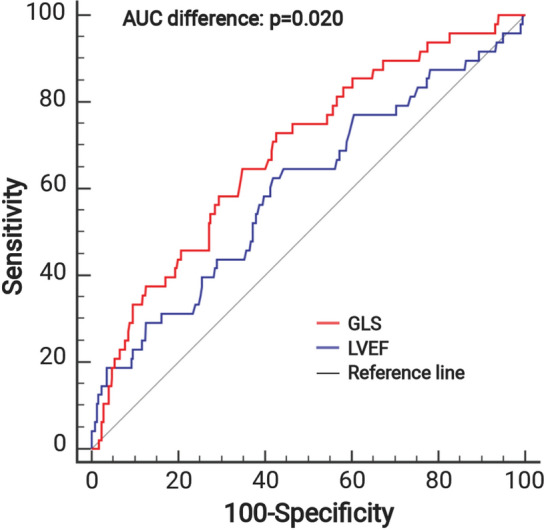
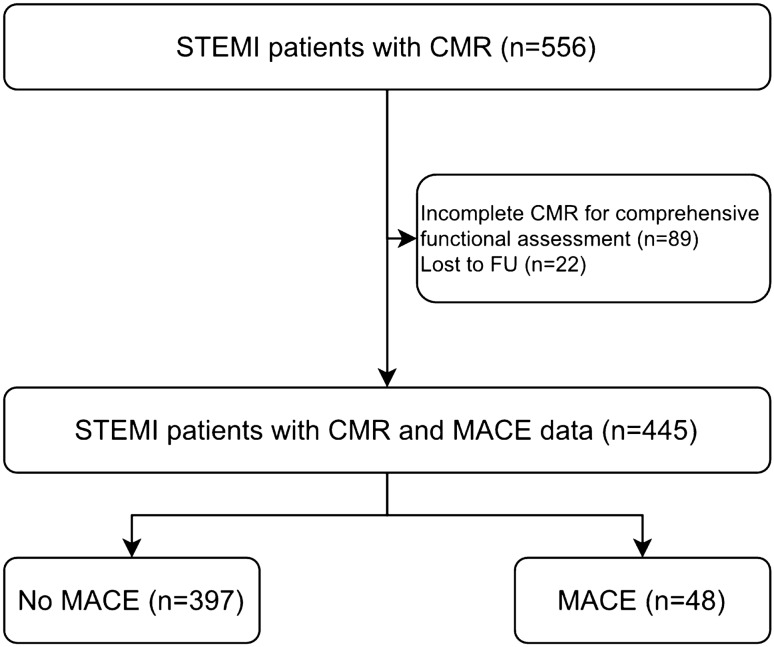
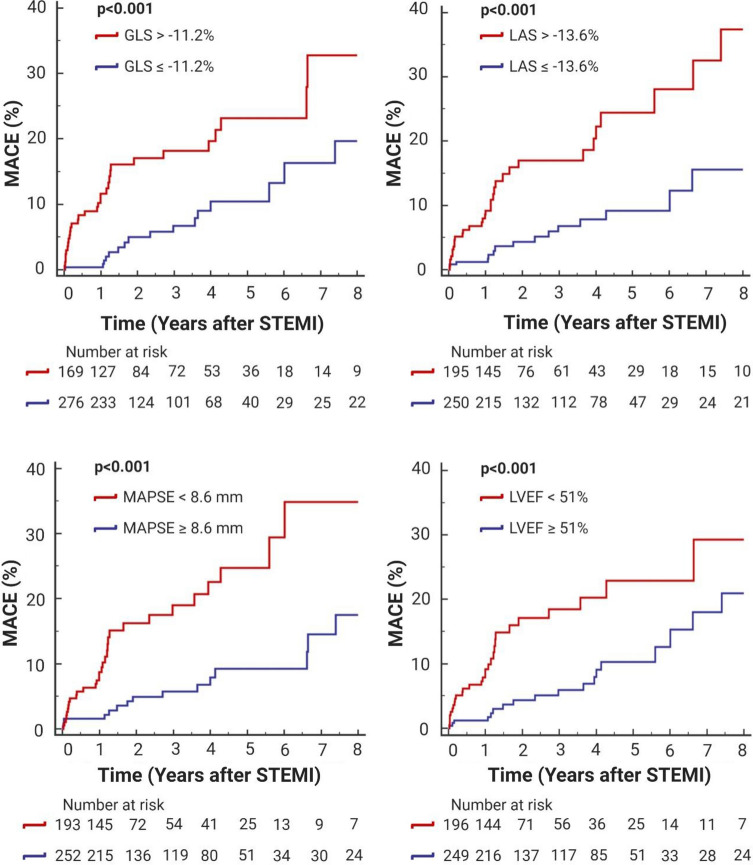
This observational cohort study included 445 acute STEMI patients treated with primary percutaneous coronary intervention (pPCI). Comprehensive CMR examinations were performed 3 [interquartile range (IQR): 2-4] days after pPCI for the determination of left ventricular (LV) functional parameters and infarct characteristics. Primary endpoint was the occurrence of major adverse cardiac events (MACE) defined as composite of death, re-infarction and congestive heart failure. During a follow-up of 16 [IQR: 12-49] months, 48 (11%) patients experienced a MACE. LVEF (p = 0.023), MAPSE (p < 0.001), LAS (p < 0.001) and GLS (p < 0.001) were significantly related to MACE. According to receiver operating characteristic analyses, only the area under the curve (AUC) of GLS was significantly higher compared to LVEF (0.69, 95% confidence interval (CI) 0.64-0.73; p < 0.001 vs. 0.60, 95% CI 0.55-0.65; p = 0.031. AUC difference: 0.09, p = 0.020). After multivariable analysis, GLS emerged as independent predictor of MACE even after adjustment for LV function, infarct size and microvascular obstruction (hazard ratio (HR): 1.13, 95% CI 1.01-1.27; p = 0.030), as well as angiographical (HR: 1.13, 95% CI 1.01-1.28; p = 0.037) and clinical parameters (HR: 1.16, 95% CI 1.05-1.29; p = 0.003).
GLS emerged as independent predictor of MACE after adjustment for parameters of LV function and myocardial damage as well as angiographical and clinical characteristics with superior prognostic validity compared to LVEF.
我们旨在研究心脏磁共振成像(CMR)测定的左心室射血分数(LVEF)、二尖瓣环平面收缩期位移(MAPSE)、快速手动长轴应变(LAS)和整体纵向应变(GLS)对ST段抬高型心肌梗死(STEMI)患者的比较预后价值。
这项观察性队列研究纳入了445例行直接经皮冠状动脉介入治疗(pPCI)的急性STEMI患者。在pPCI术后3天[四分位数间距(IQR):2 - 4天]进行全面的CMR检查,以测定左心室(LV)功能参数和梗死特征。主要终点是主要不良心脏事件(MACE)的发生,定义为死亡、再梗死和充血性心力衰竭的复合事件。在16个月[IQR:12 - 49个月]的随访期间,48例(11%)患者发生了MACE。LVEF(p = 0.023)、MAPSE(p < 0.001)、LAS(p < 0.001)和GLS(p < 0.001)与MACE显著相关。根据受试者工作特征分析,与LVEF相比,只有GLS的曲线下面积(AUC)显著更高(0.69,95%置信区间(CI)0.64 - 0.73;与0.60,95% CI 0.55 - 0.65相比,p < 0.001对p = 0.031。AUC差异:0.09,p = 0.020)。多变量分析后,即使在调整左心室功能、梗死面积和微血管阻塞后,GLS仍是MACE的独立预测因子(风险比(HR):1.13,95% CI 1.01 - 1.27;p = 0.030),以及血管造影(HR:1.13,95% CI 1.01 - 1.28;p = 0.037)和临床参数(HR:1.16,95% CI 1.05 - 1.29;p = 0.003)。
在调整左心室功能和心肌损伤参数以及血管造影和临床特征后,GLS成为MACE的独立预测因子,与LVEF相比具有更好的预后有效性。