Lebow Jocelyn, Mattke Angela, Narr Cassandra, Partain Paige, Breland Renee, Gewirtz O'Brien Janna R, Geske Jennifer, Billings Marcie, Clark Matthew M, Jacobson Robert M, Phelan Sean, Harbeck-Weber Cynthia, Le Grange Daniel, Sim Leslie
Department of Psychiatry and Psychology, Mayo Clinic School of Medicine, 200 First Street SW, Rochester, MN, 55905, USA.
Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Rochester, MN, USA.
J Eat Disord. 2021 Apr 23;9(1):55. doi: 10.1186/s40337-021-00413-9.
Family-Based Treatment (FBT) is considered the first-line intervention for adolescent anorexia nervosa. However, access to this treatment is limited. Treatment programs for other pediatric mental health conditions have successfully overcome barriers to accessing evidence-based intervention by integrating mental health services into primary care. This study evaluated the proof-of-concept of a novel modification of FBT, Family-Based Treatment for Primary Care (FBT-PC) for adolescent restrictive eating disorders designed for delivery by primary care providers in their practices.
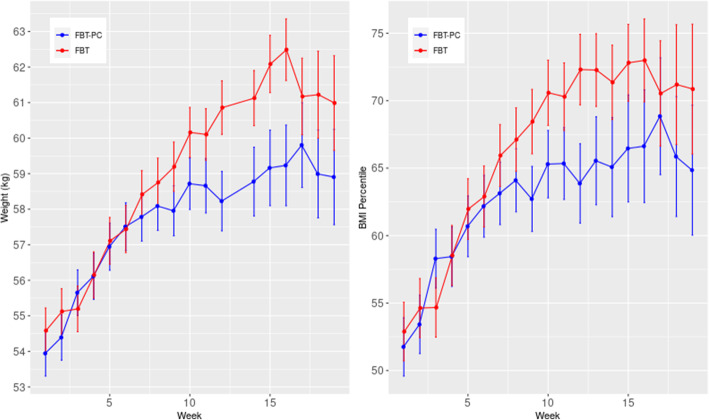
This retrospective clinical cohort study evaluated 15 adolescents with restrictive eating disorders receiving FBT-PC and 15 adolescents receiving standard FBT. We examined improvement in BMI percentile, reduction in weight suppression, and clinical benchmarks of eating disorder recovery including weight restoration to > 95% of expected body weight (EBW) and resolution of DSM-5 criteria for eating disorders.
In both groups, effect sizes for increased BMI percentile exceeded Cohen's convention for a large effect (FBT-PC: d = .94; standard FBT: d = 1.15) as did effect sizes for reduction in weight suppression (FBT-PC: d = 1.83; standard FBT: d = 1.21). At the end of treatment, 80% of the FBT-PC cohort and 87% in the standard FBT group achieved > 95%EBW and 67% in the FBT-PC group and 60% in the standard FBT group no longer met DSM-5 criteria for an eating disorder. There were no cohort differences in the number of treatment drop-outs or referrals to a more intensive level of eating disorder treatment.
Findings suggest that primary care providers have potential to improve weight and clinical status in adolescents with restrictive eating disorders. Based on these results, more rigorous testing of the FBT-PC model is warranted.
基于家庭的治疗(FBT)被认为是青少年神经性厌食症的一线干预措施。然而,获得这种治疗的机会有限。其他儿科心理健康状况的治疗项目通过将心理健康服务纳入初级保健,成功克服了获得循证干预的障碍。本研究评估了一种新型改良的FBT——初级保健家庭治疗(FBT-PC)的概念验证,该治疗专为初级保健提供者在其实践中为青少年限制性饮食障碍提供服务而设计。
这项回顾性临床队列研究评估了15名接受FBT-PC的限制性饮食障碍青少年和15名接受标准FBT的青少年。我们检查了体重指数百分位数的改善情况、体重抑制的降低情况以及饮食障碍康复的临床指标,包括体重恢复到预期体重(EBW)的>95%以及符合《精神疾病诊断与统计手册》第5版(DSM-5)饮食障碍标准的情况得到解决。
在两组中,体重指数百分位数增加的效应量超过了科恩关于大效应的标准(FBT-PC:d = 0.94;标准FBT:d = 1.15),体重抑制降低的效应量也是如此(FBT-PC:d = 1.83;标准FBT:d = 1.21)。在治疗结束时,FBT-PC队列中的80%和标准FBT组中的87%实现了>95%EBW,FBT-PC组中的67%和标准FBT组中的60%不再符合DSM-5饮食障碍标准。在治疗退出人数或转诊至更强化的饮食障碍治疗水平方面,两组之间没有差异。
研究结果表明,初级保健提供者有潜力改善患有限制性饮食障碍青少年的体重和临床状况。基于这些结果,有必要对FBT-PC模型进行更严格的测试。