Department of Cardiology, NHFPC Key Laboratory of Cardiovascular Molecular Biology and Regulatory Peptides, Peking University Third Hospital, 49 Huayuan North Road, Haidian District, Beijing, 100191, China.
Sci Rep. 2021 Apr 23;11(1):8842. doi: 10.1038/s41598-021-87953-x.
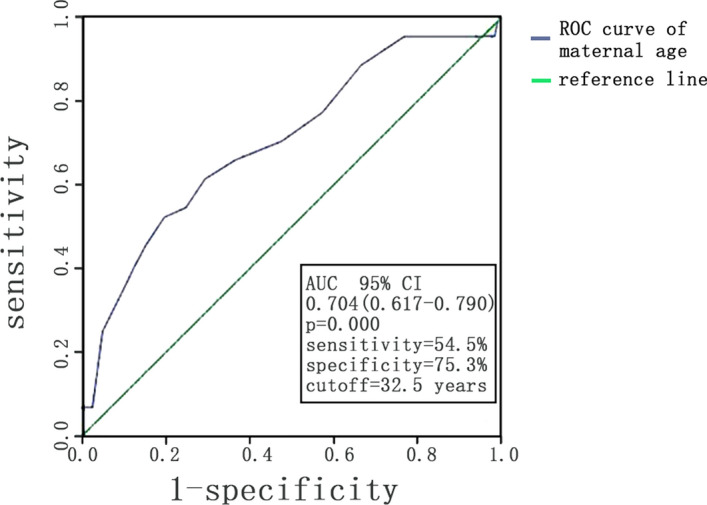
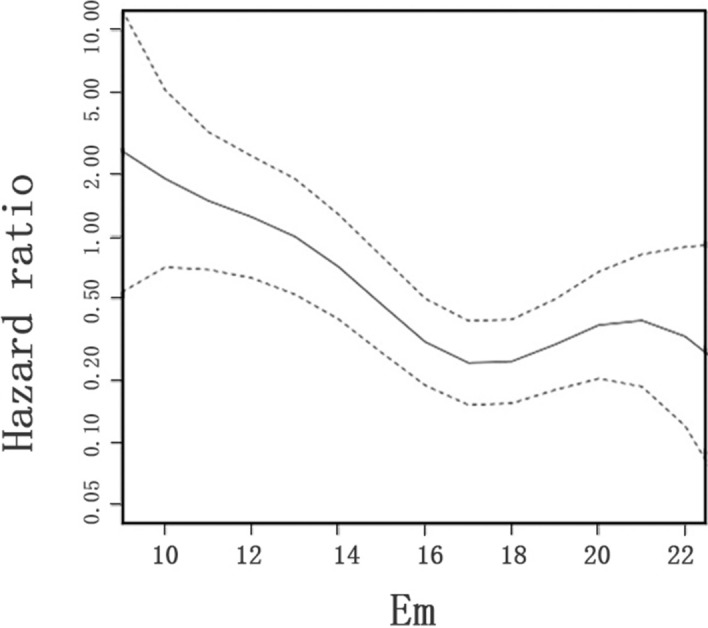
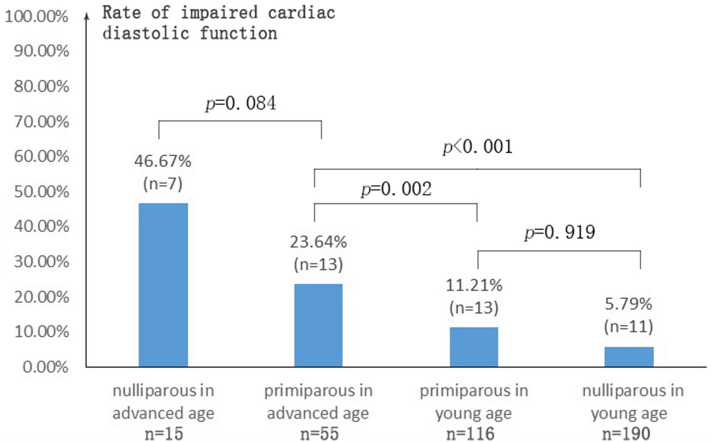
To evaluate the effect of age and parity on maternal cardiac diastolic function in second trimester among pregnant women with normal left ventricular ejection fraction. To analyze the correlation between impaired diastolic function and pre-eclampsia. It had been suggested that maternal cardiac adaptations during pregnancy differed between nulliparous and primiparous women and also varied according to age. Impaired cardiac function may precede pre-eclampsia. Therefore, we examined the effects of parity and age on cardiac diastolic function during pregnancy and whether impaired diastolic function during the second trimester correlates with pre-eclampsia. Women with singleton pregnancies at 13 + 0 to 27 + 6 weeks' gestation and left ventricular ejection fraction (LVEF) ≥ 50% were retrospectively identified. Diastolic function parameters were assessed using transthoracic echocardiography. Pre-eclampsia was identified from medical records. The effect of age and parity on maternal cardiac diastolic function as well as the correlation between impaired diastolic function and occurrence rate of pre-eclampsia were examined. 376 pregnant women were included (median age: 30 years; median gestational age: 14 weeks; 171 primiparous women). LVEF was 66%. Impaired cardiac diastolic function was seen in 7.8% of pregnant women < 35 years compared with 28.6% of those ≥ 35 years (p = 0.000). ROC curve showed women with maternal age over 32 began to have a higher rate of impaired cardiac diastolic function (AUC = 0.704, p = 0.000, sensitivity = 54.5%, specificity = 75.3%). There was no difference in diastolic function indices between maternal women grouped by parity. Higher maternal age was an independent risk factor of declining Em (p < 0.05). Em < 13 cm/s was significantly associated with pre-eclampsia occurrence (HR 8.56; 95% CI 3.40-21.57) after being adjusted for confounders. Maternal age is an independent risk factor for diastolic function decline. There is no difference in cardiac diastolic function between nulliparous women and primiparous women. Pre-eclampsia occurrence is significantly higher in patients with impaired diastolic function at mid-gestation. The application of risk grading using diastolic function at mid-gestation may improve the survival outcomes of pregnant women.
评估年龄和产次对左心室射血分数正常的孕妇中期妊娠母体心脏舒张功能的影响。分析舒张功能障碍与子痫前期的相关性。有研究表明,孕妇在怀孕期间的心脏适应性在初产妇和经产妇之间不同,而且还根据年龄而有所不同。心脏功能障碍可能先于子痫前期。因此,我们检查了产次和年龄对妊娠期间心脏舒张功能的影响,以及中期妊娠舒张功能障碍与子痫前期的相关性。回顾性确定了 13+0 至 27+6 周妊娠且左心室射血分数(LVEF)≥50%的单胎妊娠妇女。使用经胸超声心动图评估舒张功能参数。从病历中确定子痫前期。检查年龄和产次对母体心脏舒张功能的影响,以及舒张功能障碍与子痫前期发生率之间的相关性。共纳入 376 名孕妇(中位年龄:30 岁;中位孕龄:14 周;171 名初产妇)。LVEF 为 66%。与<35 岁的孕妇(7.8%)相比,≥35 岁的孕妇(28.6%)舒张功能障碍更为常见(p=0.000)。ROC 曲线显示,年龄超过 32 岁的孕妇舒张功能障碍发生率更高(AUC=0.704,p=0.000,敏感性=54.5%,特异性=75.3%)。按产次分组的孕妇舒张功能指标无差异。较高的母亲年龄是 Em 下降的独立危险因素(p<0.05)。校正混杂因素后,Em<13cm/s 与子痫前期发生显著相关(HR 8.56;95%CI 3.40-21.57)。母亲年龄是舒张功能下降的独立危险因素。初产妇和经产妇的心脏舒张功能无差异。中期妊娠舒张功能障碍患者子痫前期发生率显著升高。在中期妊娠使用舒张功能进行风险分级的应用可能会改善孕妇的生存结局。