Department of Surgery, University of Pittsburgh, Pittsburgh, Pennsylvania, USA.
Department of Surgery and Epidemiology, University of Pittsburgh, Pittsburgh, Pennsylvania, USA.
J Surg Oncol. 2021 Sep;124(3):308-316. doi: 10.1002/jso.26510. Epub 2021 Apr 24.
Neoadjuvant chemotherapy (NAT) for pancreatic adenocarcinoma (PDAC) is increasingly being utilized. However, a significant number of patients will experience early recurrence, possibly negating the benefit of surgery. We aimed to identify factors implicated in early disease recurrence.
A retrospective review of pancreaticoduodenectomies performed between 2005 and 2017 at our institution for PDAC following NAT was performed. A 6-month cut-off was used to stratify patients into early/late recurrence groups. Multivariate analysis was performed to identify predictors of recurrence.
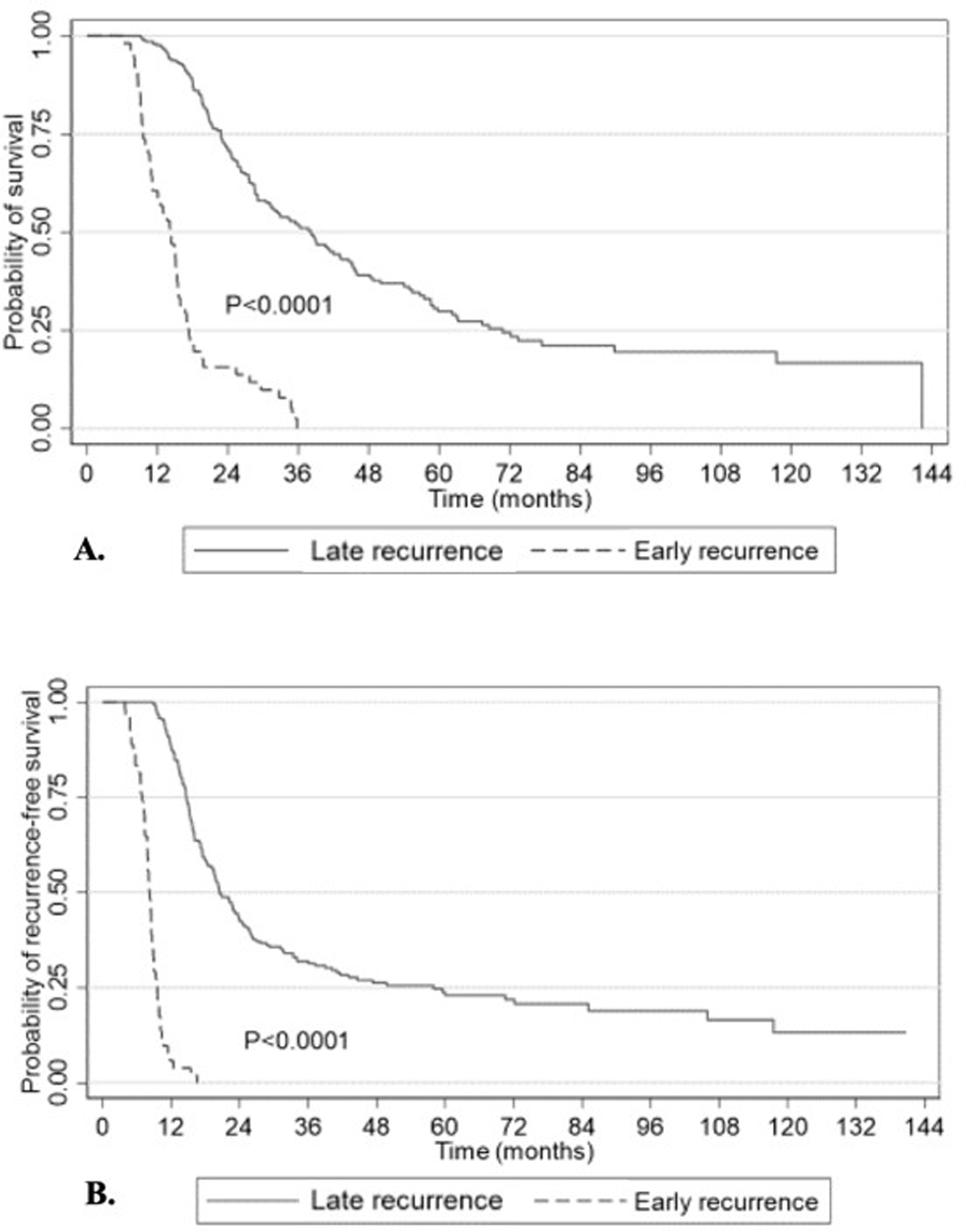
Of 273 patients, 64 (23%) developed early recurrence or died within 90 days of surgery. The median time to recurrence was 4 months (95% confidence interval [CI]: 2.2-4.3) in the early group versus 16 months (95% CI: 13.7-19.9) in the late group. The former had higher baseline and post-NAT Ca19-9 levels than the latter (472 vs. 153 IU/ml, p = 0.001 and 71 vs. 39 IU/ml, p = 0.005, respectively). A higher positive lymph node ratio significantly increased the risk of early recurrence (hazard ratio [HR]: 15.9, p < 0.001) while adjuvant chemotherapy was protective (HR: 0.4, p < 0.001).
Our findings acknowledge the limitations of clinically measured factors used to ascertain response to NAT and underline the need for individualized molecular markers that take into consideration the specific tumor biology.
新辅助化疗(NAT)在胰腺腺癌(PDAC)中的应用日益增多。然而,大量患者将经历早期复发,这可能使手术受益化为泡影。我们旨在确定与早期疾病复发相关的因素。
我们对 2005 年至 2017 年期间在我院接受 NAT 后行胰十二指肠切除术的 PDAC 患者进行了回顾性研究。我们使用 6 个月的时间截点将患者分为早期/晚期复发组。进行多变量分析以确定复发的预测因素。
在 273 例患者中,有 64 例(23%)在术后 90 天内出现早期复发或死亡。早期复发组的中位复发时间为 4 个月(95%置信区间:2.2-4.3),晚期复发组为 16 个月(95%置信区间:13.7-19.9)。前者的基线和 NAT 后 CA19-9 水平均高于后者(472 vs. 153 IU/ml,p=0.001 和 71 vs. 39 IU/ml,p=0.005)。较高的阳性淋巴结比值显著增加了早期复发的风险(风险比 [HR]:15.9,p<0.001),而辅助化疗则具有保护作用(HR:0.4,p<0.001)。
我们的研究结果承认了用于确定 NAT 反应的临床测量因素的局限性,并强调需要个体化的分子标志物,以考虑到特定的肿瘤生物学。