Public Health France, Saint-Maurice, France.
APEx Collaboration for Academic Primary Care, Health Services and Policy Research Group, University of Exeter, Exeter, United Kingdom.
PLoS Med. 2021 Apr 26;18(4):e1003584. doi: 10.1371/journal.pmed.1003584. eCollection 2021 Apr.
Given the increasing burden of chronic conditions, multimorbidity is now a priority for healthcare and public health systems worldwide. Appropriate methodological approaches for assessing the phenomenon have not yet been established, resulting in inconsistent and incomplete descriptions. We aimed to estimate and characterize the burden of multimorbidity in the adult population in France in terms of number and type of conditions, type of underlying mechanisms, and analysis of the joint effects for identifying combinations with the most deleterious interaction effects on health status.
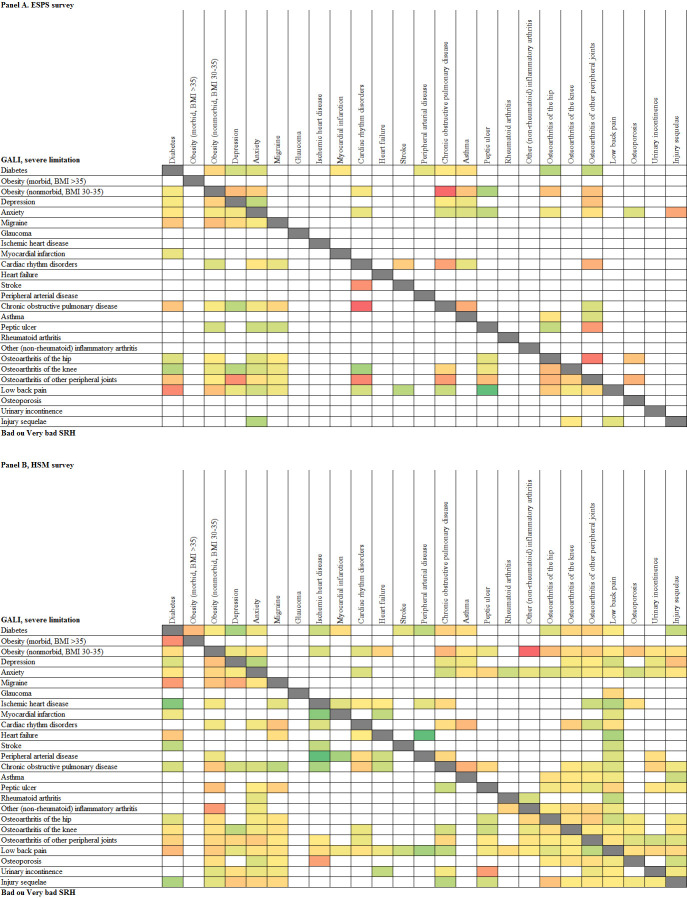
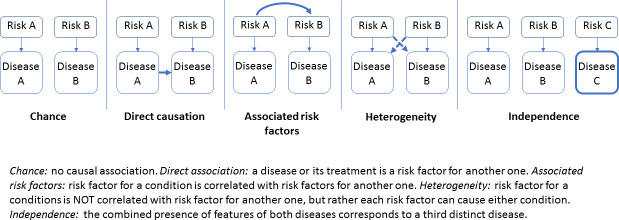
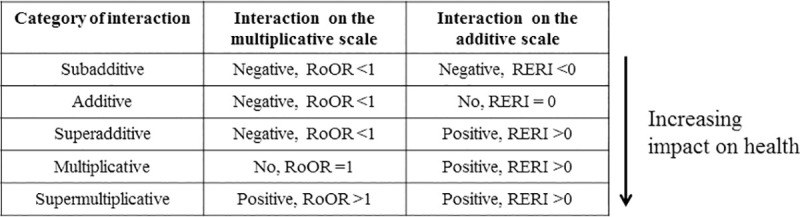
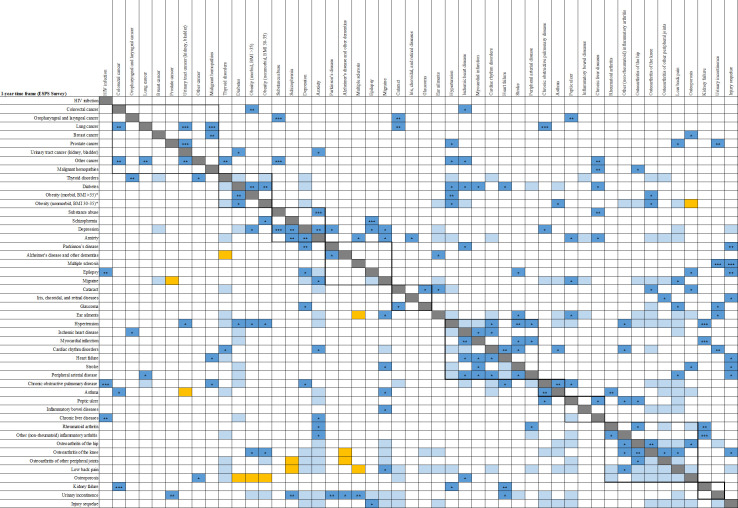
We used a multistep approach to analyze cross-sectional and longitudinal data from 2 large nationwide representative surveys: 2010/2014 waves of the Health, Health Care, and Insurance Survey (ESPS 2010-2014) and Disability Healthcare Household Survey 2008 (HSM 2008), that collected similar data on 61 chronic or recurrent conditions. Adults aged ≥25 years in either ESPS 2010 (14,875) or HSM 2008 (23,348) were considered (participation rates were 65% and 62%, respectively). Longitudinal analyses included 7,438 participants of ESPS 2010 with follow-up for mortality (97%) of whom 3,798 were reinterviewed in 2014 (52%). Mortality, activity limitation, self-reported health, difficulties in activities/instrumental activities of daily living, and Medical Outcomes Study Short-Form 12-Item Health Survey were the health status measures. Multiple regression models were used to estimate the impact of chronic or recurrent conditions and multimorbid associations (dyads, triads, and tetrads) on health status. Etiological pathways explaining associations were investigated, and joint effects and interactions between conditions on health status measures were evaluated using both additive and multiplicative scales. Forty-eight chronic or recurrent conditions had an independent impact on mortality, activity limitations, or perceived heath. Multimorbidity prevalence varied between 30% (1-year time frame) and 39% (lifetime frame), and more markedly according to sex (higher in women), age (with greatest increases in middle-aged), and socioeconomic status (higher in less educated and low-income individuals and manual workers). We identified various multimorbid combinations, mostly involving vasculometabolic and musculoskeletal conditions and mental disorders, which could be explained by direct causation, shared or associated risk factors, or less frequently, confounding or chance. Combinations with the highest health impacts included diseases with complications but also associations of conditions affecting systems involved in locomotion and sensorial functions (impact on activity limitations), and associations including mental disorders (impact on perceived health). The interaction effects of the associated conditions varied on a continuum from subadditive and additive (associations involving cardiometabolic conditions, low back pain, osteoporosis, injury sequelae, depression, and anxiety) to multiplicative and supermultiplicative (associations involving obesity, chronic obstructive pulmonary disease, migraine, and certain osteoarticular pathologies). Study limitations included self-reported information on chronic conditions and the insufficient power of some analyses.
Multimorbidity assessments should move beyond simply counting conditions and take into account the variable impacts on health status, etiological pathways, and joint effects of associated conditions. In particular, the multimorbid combinations with substantial health impacts or shared risk factors deserve closer attention. Our findings also suggest that multimorbidity assessment and management may be beneficial already in midlife and probably earlier in disadvantaged groups.
鉴于慢性病负担不断增加,全球医疗和公共卫生系统现在将多种疾病作为优先事项。尚未建立适当的方法来评估这一现象,导致描述不一致且不完整。我们旨在根据疾病数量和类型、潜在机制类型以及联合效应分析来估计和描述法国成年人群中多种疾病的负担,以识别对健康状况具有最不利交互效应的组合。
我们使用多步骤方法分析了两项全国代表性调查的横断面和纵向数据:2010/2014 年健康、医疗保健和保险调查(ESPS 2010-2014)和 2008 年残疾医疗保健家庭调查(HSM 2008),这些调查收集了类似的 61 种慢性或复发性疾病的数据。年龄≥25 岁的 ESPS 2010(14875 人)或 HSM 2008(23348 人)的参与者被认为是符合条件的(参与率分别为 65%和 62%)。纵向分析包括 ESPS 2010 中的 7438 名参与者,对其中 97%的人进行了随访以评估死亡率,其中 3798 人在 2014 年再次接受了随访(52%)。死亡率、活动受限、自我报告的健康状况、活动和工具性日常生活活动困难以及医疗结局研究短量表 12 项健康调查是健康状况的衡量指标。使用多元回归模型来估计慢性或复发性疾病以及多种疾病关联(二元、三元和四元)对健康状况的影响。研究了解释关联的病因途径,并使用加性和乘法尺度评估了疾病之间的联合效应和相互作用对健康状况衡量指标的影响。48 种慢性或复发性疾病对死亡率、活动受限或自我感知健康有独立影响。多种疾病的患病率在 30%(1 年时间范围)到 39%(终生范围)之间变化,且根据性别(女性更高)、年龄(中年时增加最大)和社会经济地位(受教育程度较低和低收入个体以及体力劳动者更高)而有更大差异。我们确定了各种多种疾病的组合,主要涉及血管代谢和肌肉骨骼疾病以及精神障碍,这些可以通过直接因果关系、共同或相关的危险因素来解释,或者不太常见的是,通过混杂或机会来解释。对健康影响最大的组合包括有并发症的疾病以及影响运动和感觉功能系统的疾病的关联(对活动受限的影响),以及包括精神障碍的关联(对自我感知健康的影响)。关联疾病的相互作用效应在加性和(涉及心血管代谢疾病、下背痛、骨质疏松症、创伤后遗症、抑郁和焦虑的关联)与乘法和超乘法(涉及肥胖症、慢性阻塞性肺疾病、偏头痛和某些骨关节炎疾病的关联)之间连续变化。研究的局限性包括对慢性疾病的自我报告信息以及某些分析的能力不足。
多种疾病的评估不应仅仅停留在计数疾病的层面上,而应考虑对健康状况的可变影响、病因途径以及关联疾病的联合效应。特别是,具有重大健康影响或共同危险因素的多种疾病组合值得更密切关注。我们的研究结果还表明,多种疾病的评估和管理可能在中年甚至在弱势群体中更早受益。