Department of Surgery, Renaissance School of Medicine, HSC T-12, Room 064, Stony Brook, NY, 11794, USA.
Department of Neurosurgery, Renaissance School of Medicine, Stony Brook, NY, USA.
J Gastrointest Surg. 2022 Jan;26(1):181-190. doi: 10.1007/s11605-021-05015-z. Epub 2021 Apr 27.
Although acute gastrointestinal injury (AGI) and feeding intolerance (FI) are known independent determinants of worse outcomes and high mortality in intensive care unit (ICU) patients, the incidence of AGI and FI in critically ill COVID-19 patients and their prognostic importance have not been thoroughly studied.
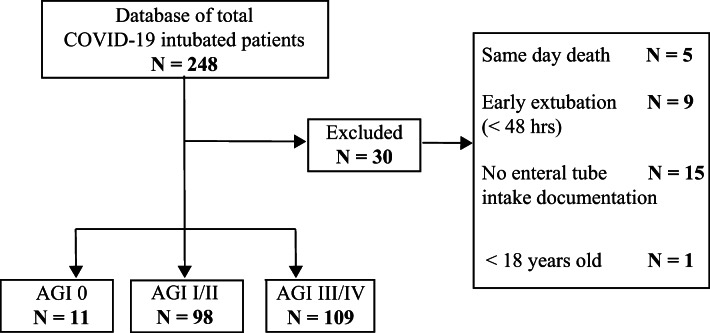
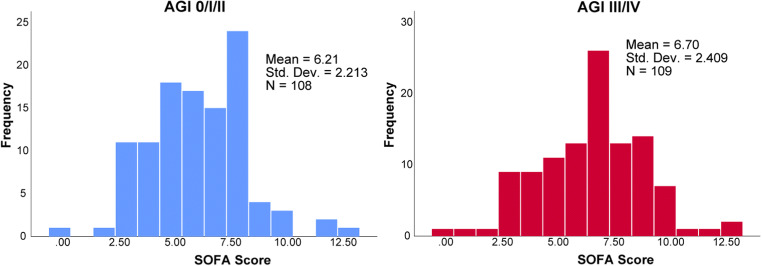
We reviewed 218 intubated patients at Stony Brook University Hospital and stratified them into three groups based on AGI severity, according to data collected in the first 10 days of ICU course. We used chi-square test to compare categorical variables such as age and sex and two-sample t-test or Mann-Whitney U-tests for continuous variables, including important laboratory values. Cox proportional hazards regression models were utilized to determine whether AGI score was an independent predictor of survival, and multivariable analysis was performed to compare risk factors that were deemed significant in the univariable analysis. We performed Kaplan-Meier survival analysis based on the AGI score and the presence of FI.
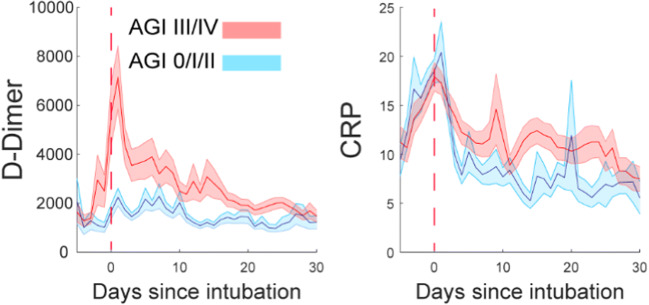
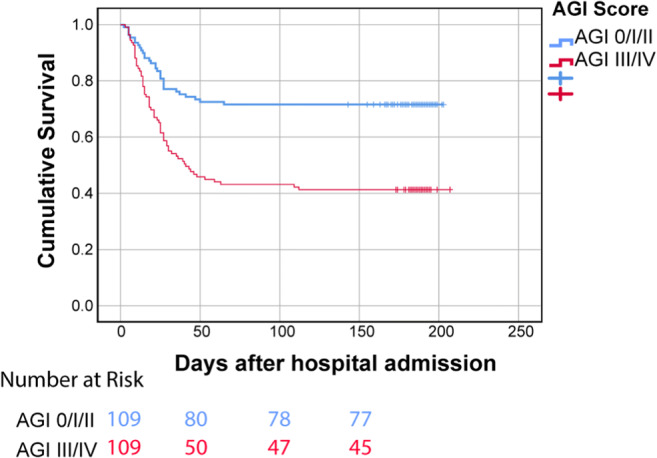
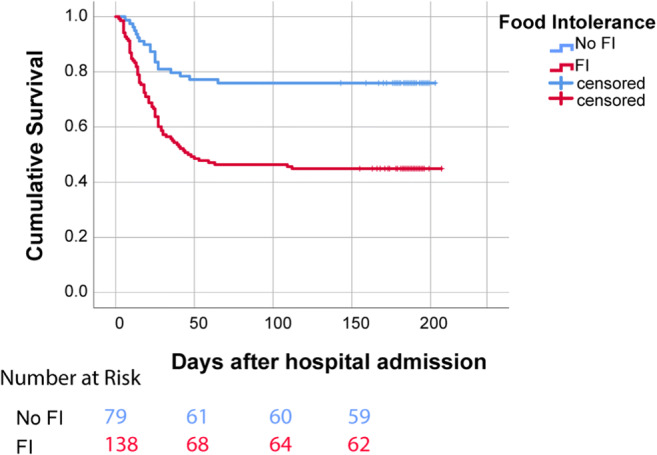
The overall incidence of AGI was 95% (45% AGI I/II, 50% AGI III/IV), and FI incidence was 63%. Patients with AGI III/IV were more likely to have prolonged mechanical ventilation (22 days vs 16 days, P-value <0.002) and higher mortality rate (58% vs 28%, P-value <0.001) compared to patients with AGI 0/I/II. This was confirmed with multivariable analysis which showed that AGI score III/IV was an independent predictor of higher mortality (AGI III/IV vs AGI 0/I/II hazard ratio (HR), 2.68; 95% confidence interval (CI), 1.69-4.25; P-value <0.0001). Kaplan-Meier survival analysis showed that both AGI III/IV and FI (P-value <0.001) were associated with worse outcomes. Patients with AGI III/IV had higher daily and mean D-dimer and CRP levels compared to AGI 0/I/II (P-value <0.0001).
The prevalence of AGI and FI among critically ill COVID-19 patients was high. AGI grades III/IV were associated with higher risk for prolonged mechanical ventilation and mortality compared to AGI 0/I/II, while it also correlated with higher D-dimer and C-reactive protein (CRP) levels. FI was independently associated with higher mortality. The development of high-grade AGI and FI during the first days of ICU stay can serve as prognostic tools to predict outcomes in critically ill COVID-19 patients.
尽管急性胃肠损伤(AGI)和喂养不耐受(FI)是重症监护病房(ICU)患者预后不良和高死亡率的独立决定因素,但危重症 COVID-19 患者中 AGI 和 FI 的发生率及其预后意义尚未得到充分研究。
我们回顾了石溪大学医院 218 例插管患者,并根据 ICU 病程前 10 天收集的数据,根据 AGI 严重程度将其分为三组。我们使用卡方检验比较了年龄和性别等分类变量,使用两样本 t 检验或 Mann-Whitney U 检验比较了重要的实验室值等连续变量。我们使用 Cox 比例风险回归模型来确定 AGI 评分是否是生存的独立预测因子,并进行多变量分析以比较单变量分析中认为重要的危险因素。我们根据 AGI 评分和 FI 的存在进行了 Kaplan-Meier 生存分析。
AGI 的总发生率为 95%(45% AGI I/II,50% AGI III/IV),FI 的发生率为 63%。与 AGI 0/I/II 患者相比,AGI III/IV 患者更有可能需要长时间机械通气(22 天与 16 天,P 值<0.002)和死亡率更高(58%与 28%,P 值<0.001)。多变量分析证实了这一点,结果表明 AGI 评分 III/IV 是死亡率较高的独立预测因子(AGI III/IV 与 AGI 0/I/II 的危险比(HR),2.68;95%置信区间(CI),1.69-4.25;P 值<0.0001)。Kaplan-Meier 生存分析表明,AGI III/IV 和 FI(P 值<0.001)均与不良结局相关。与 AGI 0/I/II 相比,AGI III/IV 患者的每日和平均 D-二聚体和 C 反应蛋白(CRP)水平更高(P 值<0.0001)。
危重症 COVID-19 患者中 AGI 和 FI 的发生率较高。与 AGI 0/I/II 相比,AGI III/IV 与更长时间的机械通气和死亡率增加相关,而与更高的 D-二聚体和 CRP 水平相关。FI 与死亡率增加独立相关。在 ICU 入住的最初几天内发生高级 AGI 和 FI 可作为预测危重症 COVID-19 患者结局的预后工具。