Sorbonne Université, INSERM, Centre d'Immunologie et des Maladies Infectieuses (CIMI-Paris).
Assistance Publique-Hôpitaux de Paris, Sorbonne Université, Department of Infectious Diseases, Pitie-Salpetriere Hospital, Pierre Louis Institute of Epidemiology and Public Health, Sorbonne Université, Paris.
Medicine (Baltimore). 2021 Apr 30;100(17):e25678. doi: 10.1097/MD.0000000000025678.
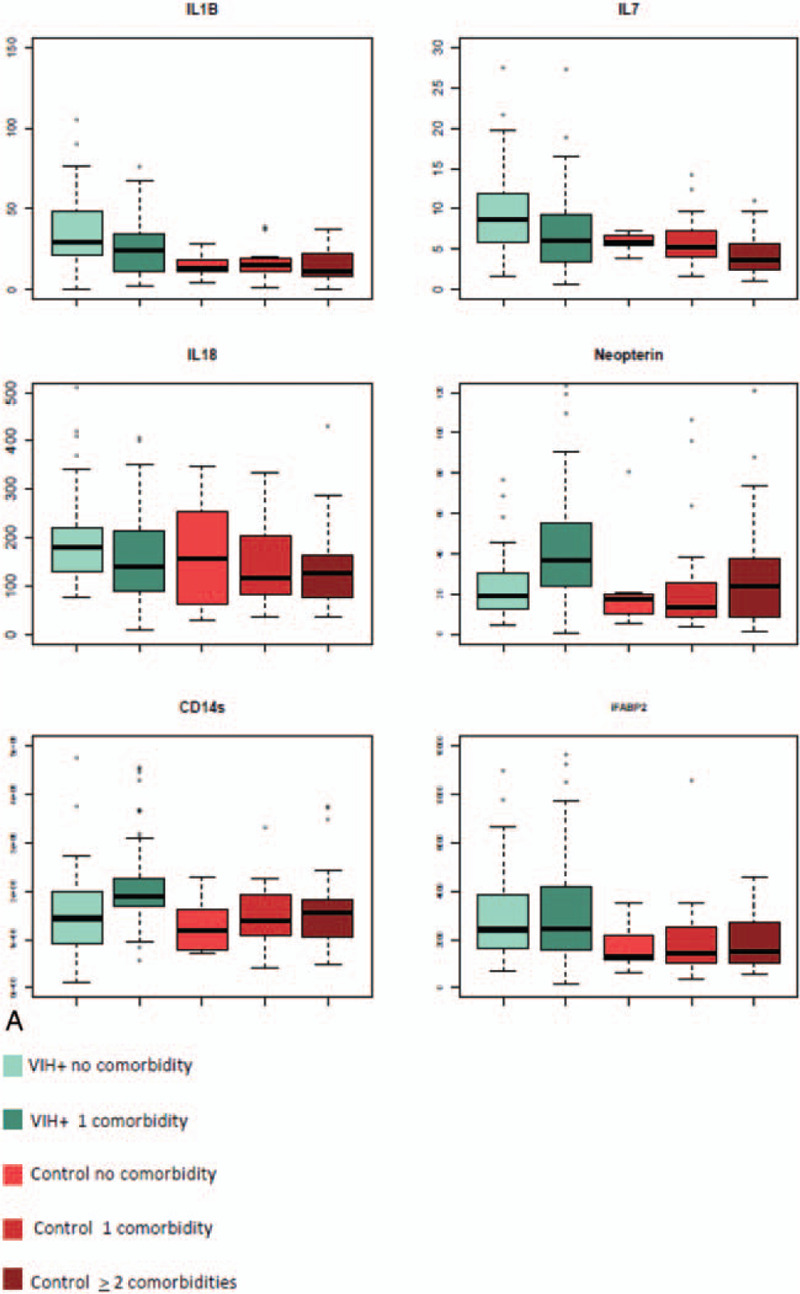
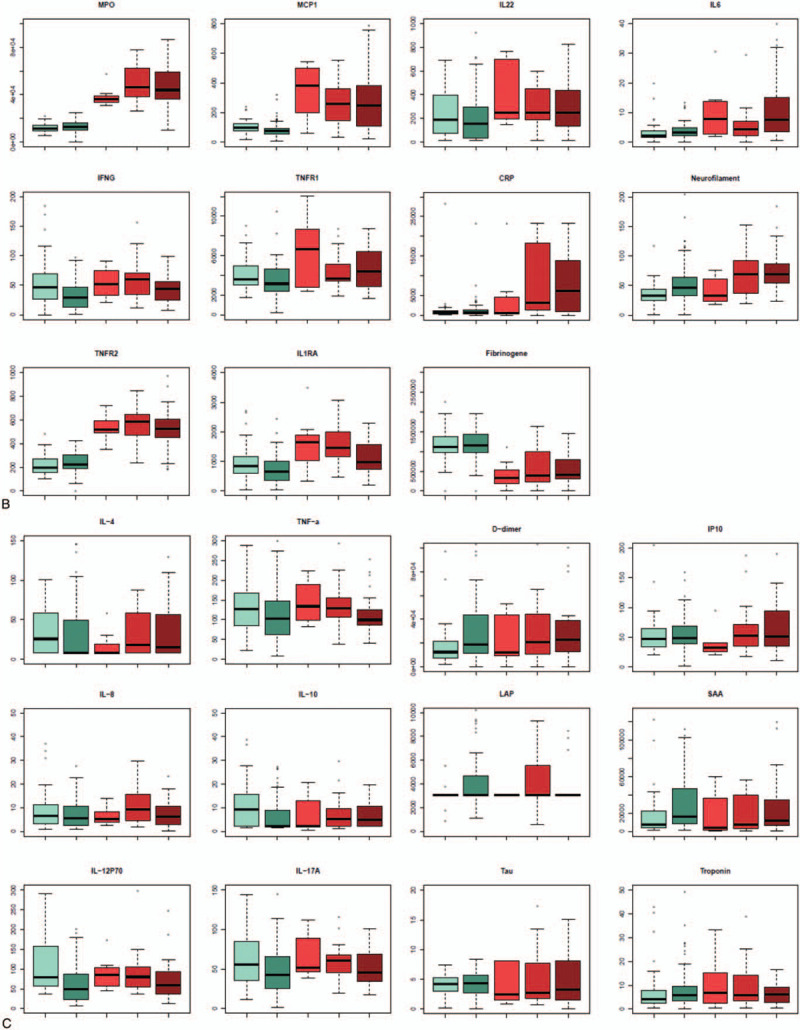
HIV infection has become a chronic disease, with a lower mortality, but a consequent increase in age-related noninfectious comorbidities. Metabolic disorders have been linked to the effect of cART as well to the effects of immune activation and chronic inflammation. Whereas it is known that aging is intrinsically associated with hyperinflammation and immune system deterioration, the relative impact of chronic HIV infection on such inflammatory and immune activation has not yet been studied focusing on an elderly HIV-infected population.The objectives of the study were to assess 29 blood markers of immune activation and inflammation using an ultrasensitive technique, in HIV-infected patients aged ≥75 years with no or 1 comorbidity (among hypertension, renal disease, neoplasia, diabetes mellitus, cardiovascular disease, stroke, dyslipidemia, and osteoporosis), in comparison with age-adjusted HIV-uninfected individuals to identify whether biomarkers were associated with comorbidities. Wilcoxon nonparametric tests were used to compare the levels of each marker between control and HIV groups; logistic regression to identify biomarkers associated to comorbidity in the HIV group and principal component analysis (PCA) to determine clusters associated with a group or a specific comorbidity.A total of 111 HIV-infected subjects were included from the Dat'AIDS cohort and compared to 63 HIV-uninfected controls. In the HIV-infected group, 4 biomarkers were associated with the risk of developing a comorbidity: monocyte chemoattractant protein-1 (MCP-1), neurofilament light chain (NF-L), neopterin, and soluble CD14. Six biomarkers (interleukin [IL]-1B, IL-7, IL-18, neopterin, sCD14, and fatty acid-binding protein) were significantly higher in the HIV-infected group compared to the control group, 11 biomarkers (myeloperoxydase, interleukin-1 receptor antagonist, tumor necrosis factor receptor 1, interferon-gamma, MCP-1, tumor necrosis factor receptor 2, IL-22, ultra sensitivity C-reactive protein, fibrinogen, IL-6, and NF-L) were lower. Despite those differences, PCA to determine clusters associated with a group or a specific comorbidity did not reveal clustering nor between healthy control and HIV-infected patients neither between the presence of comorbidity within HIV-infected group.In this highly selected geriatric HIV population, HIV infection does not seem to have an additional impact on age-related inflammation and immune disorder. Close monitoring could have led to optimize prevention and treatment of comorbidities, and have limited both immune activation and inflammation in the aging HIV population.
HIV 感染已成为一种慢性病,死亡率较低,但与年龄相关的非传染性合并症相应增加。代谢紊乱与 cART 的作用以及免疫激活和慢性炎症的作用有关。虽然众所周知,衰老与过度炎症和免疫系统恶化有关,但慢性 HIV 感染对这种炎症和免疫激活的相对影响尚未得到研究,特别是针对老年 HIV 感染者。本研究的目的是使用超敏技术评估 29 种免疫激活和炎症的血液标志物,这些标志物在无合并症或仅有 1 种合并症(高血压、肾脏疾病、肿瘤、糖尿病、心血管疾病、中风、血脂异常和骨质疏松症)的年龄≥75 岁的 HIV 感染者中,与年龄匹配的 HIV 未感染者进行比较,以确定生物标志物是否与合并症有关。Wilcoxon 非参数检验用于比较对照组和 HIV 组中每种标志物的水平;逻辑回归用于确定与 HIV 组中合并症相关的生物标志物,主成分分析(PCA)用于确定与组或特定合并症相关的聚类。总共从 Dat'AIDS 队列中纳入了 111 名 HIV 感染者,并与 63 名 HIV 未感染者进行了比较。在 HIV 感染者中,有 4 种生物标志物与发生合并症的风险相关:单核细胞趋化蛋白-1(MCP-1)、神经丝轻链(NF-L)、新蝶呤和可溶性 CD14。与对照组相比,HIV 感染者中有 6 种生物标志物(白细胞介素[IL]-1B、IL-7、IL-18、新蝶呤、sCD14 和脂肪酸结合蛋白)显著升高,11 种生物标志物(髓过氧化物酶、白细胞介素-1 受体拮抗剂、肿瘤坏死因子受体 1、干扰素-γ、MCP-1、肿瘤坏死因子受体 2、IL-22、超敏 C 反应蛋白、纤维蛋白原、IL-6 和 NF-L)降低。尽管存在这些差异,但 PCA 确定与组或特定合并症相关的聚类并未显示聚类,也未显示健康对照组与 HIV 感染者之间或 HIV 感染者组内合并症之间的聚类。在这个高度选择的老年 HIV 人群中,HIV 感染似乎对与年龄相关的炎症和免疫紊乱没有额外的影响。密切监测可能会优化合并症的预防和治疗,并限制老年 HIV 人群中的免疫激活和炎症。