Division of Rheumatology, Department of Medicine, University of Washington, Seattle, WA, USA.
Division of Medical Oncology, Department of Medicine, University of Washington, 1144 Eastlake Ave E, LG-465, Seattle, WA, 98109, USA.
Sci Rep. 2021 Apr 27;11(1):9029. doi: 10.1038/s41598-021-88307-3.
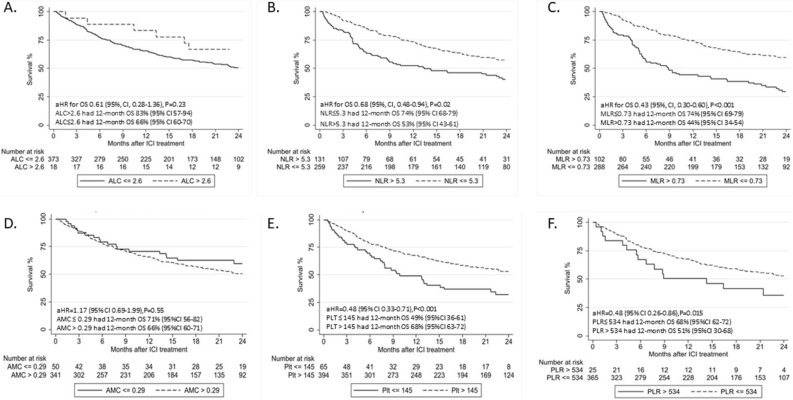
Patients with cancer treated with immune checkpoint inhibitors (ICIs) develop immune related adverse events (irAEs), however biomarkers are lacking. We hypothesized that clinicopathologic and laboratory factors would be associated with irAE risk and overall survival (OS) in this population. In a retrospective study of patients treated with ICIs we collected clinicopathologic, laboratory, irAEs and outcomes data. The association between baseline blood biomarkers, clinicopathologic features and irAEs was assessed by logistic regression adjusting for age, sex, smoking, cancer type, performance status, concomitant other systemic therapy, history of autoimmune disease (AD), chronic infection and pre-existing systemic steroid use (regardless of dose). Optimal cutoff values of biomarkers were identified by recursive partitioning analysis. 470 patients were identified; 156 (33%) developed irAEs, which were associated with baseline absolute lymphocyte count > 2.6 k/ul (adjusted [a]OR: 4.30), absolute monocyte count > 0.29 k/ul (aOR: 2.34) and platelet count > 145 k/ul (aOR: 2.23), neutrophil to lymphocyte ratio (NLR) ≤ 5.3 (aOR: 2.07) and monocyte to lymphocyte ratio (MLR) ≤ 0.73 (aOR: 2.96), as well as platelet to lymphocyte ratio ≤ 534 (aOR: 5.05). Patients with pre-existing AD (aOR: 2.57), family history of AD (aOR: 5.98), and ICI combination (aOR: 2.00) had higher odds of irAEs. Baseline NLR ≤ 5.3 (aHR: 0.68), MLR ≤ 0.73 (aHR: 0.43), PLT > 145 (aHR: 0.48) and PLR ≤ 534 (aHR: 0.48) were associated with longer OS. irAEs were associated with autoimmune history, ICI combination and baseline laboratory measurements. Lower NLR, MLR and PLR may have favorable prognostic value. Our hypothesis-generating findings require validation in larger prospective studies.
接受免疫检查点抑制剂 (ICI) 治疗的癌症患者会发生免疫相关不良反应 (irAE),但目前缺乏生物标志物。我们假设,在该人群中,临床病理和实验室因素与 irAE 风险和总生存期 (OS) 相关。在一项对接受 ICI 治疗的患者的回顾性研究中,我们收集了临床病理、实验室、irAE 和结局数据。通过调整年龄、性别、吸烟、癌症类型、表现状态、同时使用其他全身治疗、自身免疫性疾病 (AD) 史、慢性感染和预先存在的全身类固醇使用(无论剂量如何),评估基线血液生物标志物、临床病理特征与 irAE 之间的关联。通过递归分区分析确定生物标志物的最佳截断值。共确定了 470 例患者;其中 156 例 (33%) 发生了 irAE,与基线时绝对淋巴细胞计数 > 2.6k/ul (调整后的[OR]:4.30)、绝对单核细胞计数 > 0.29k/ul (OR:2.34)和血小板计数 > 145k/ul (OR:2.23)、中性粒细胞与淋巴细胞比值 (NLR)≤5.3 (OR:2.07)和单核细胞与淋巴细胞比值 (MLR)≤0.73 (OR:2.96)以及血小板与淋巴细胞比值 (PLR)≤534 (OR:5.05)相关。有预先存在的 AD (OR:2.57)、AD 家族史 (OR:5.98)和 ICI 联合治疗 (OR:2.00)的患者发生 irAE 的可能性更高。基线 NLR≤5.3 (aHR:0.68)、MLR≤0.73 (aHR:0.43)、PLT>145 (aHR:0.48)和 PLR≤534 (aHR:0.48)与更长的 OS 相关。irAE 与自身免疫史、ICI 联合治疗和基线实验室检查有关。较低的 NLR、MLR 和 PLR 可能具有有利的预后价值。我们的假设生成结果需要在更大的前瞻性研究中验证。