Department of Urology, The Jikei University School of Medicine, 3-25-8, Nishi-Shimbashi, Minato-ku, 105-8461, Tokyo, Japan.
Department of Urology, Medical University of Vienna, Vienna, Austria.
Strahlenther Onkol. 2021 Nov;197(11):976-985. doi: 10.1007/s00066-021-01784-3. Epub 2021 Apr 28.
To assess the outcomes of high-dose-rate (HDR) brachytherapy and hypofractionated external beam radiation therapy (EBRT) combined with long-term androgen deprivation therapy (ADT) in very-high-risk (VHR) versus high-risk (HR) prostate cancer (PCa), as defined in the National Comprehensive Cancer Network (NCCN) criteria.
Data from 338 consecutive HR or VHR PCa patients who had undergone this tri-modal therapy between 2005 and 2018 were retrospectively analyzed. Biochemical recurrence (BCR)-free, progression-free, overall, and cancer-specific survival (BCRFS/PFS/OS/CSS) rates were analyzed using the Kaplan-Meier method and Wilcoxon test. Cox regression models were used to evaluate candidate prognostic factors for survival. C‑indexes were used to assess model discrimination.
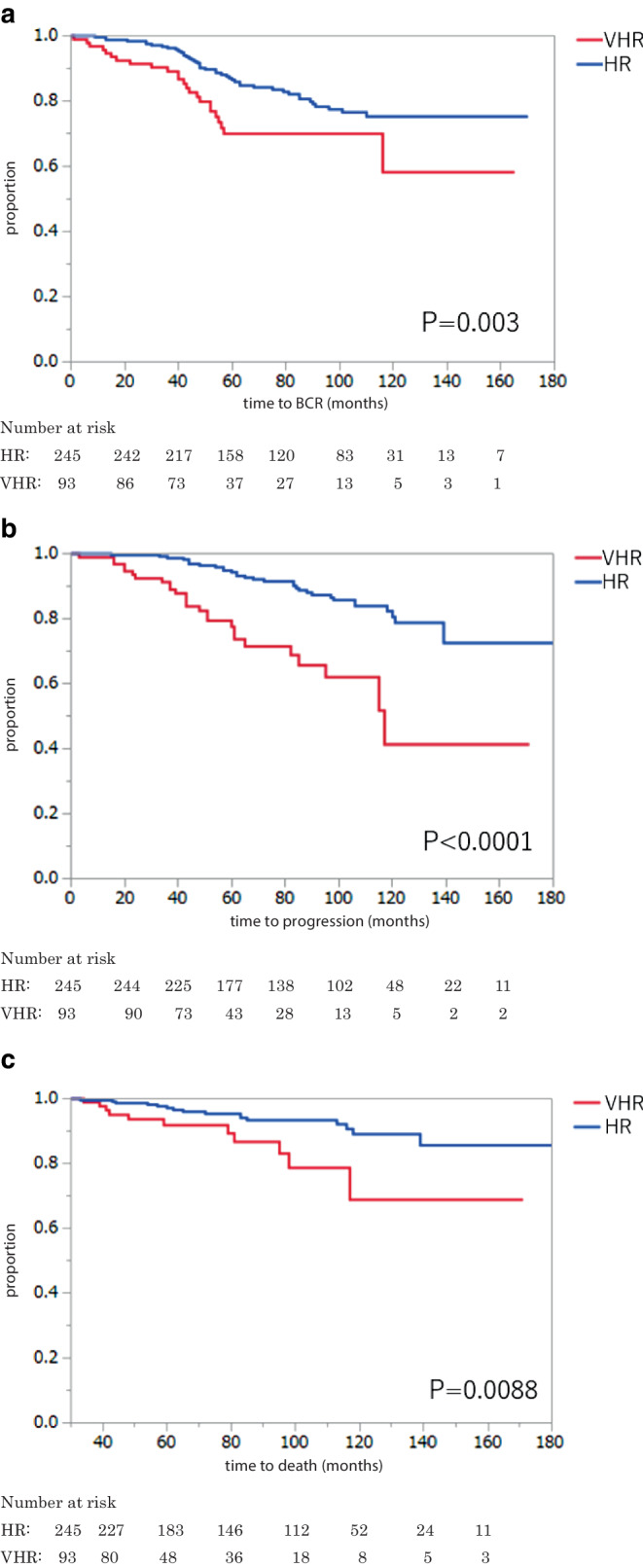
Within a median follow-up of 84 months, 68 patients experienced BCR, 58 had disease progression including only 3 with local progression, 27 died of any cause, and 2 died from PCa. The 5‑year BCRFS, PFS, OS, and CSS rates were 82.2% (HR 86.5%; VHR 70.0%), 90.0% (HR 94.3%; VHR 77.6%), 95.7% (HR, 97.1%; VHR, 91.8%), and 99.6% (HR, 100%; VHR, 98.0%), respectively. In multivariable analyses that adjusted for standard clinicopathologic features, the risk subclassification was associated both PFS and OS (p = 0.0003 and 0.001, respectively). Adding the risk subclassification improved the accuracy of models in predicting BCRFS, PFS, and OS.
While the outcome of this trimodal approach appears favorable, VHR PCa patients had significantly worse oncological outcomes than those with HR PCa. The NCCN risk subclassification should be integrated into prognostic tools to guide risk stratification, treatment, and follow-up for unfavorable PCa patients receiving this trimodal therapy.
根据美国国家综合癌症网络(NCCN)标准,评估高剂量率(HDR)近距离放疗和低分割外照射放疗(EBRT)联合长期雄激素剥夺治疗(ADT)在极高危(VHR)与高危(HR)前列腺癌(PCa)中的治疗效果。
回顾性分析了 2005 年至 2018 年间,338 例接受这种三联疗法的 HR 或 VHR PCa 患者的数据。使用 Kaplan-Meier 方法和 Wilcoxon 检验分析无生化复发(BCR)、无进展、总生存期和癌症特异性生存期(BCRFS/PFS/OS/CSS)。Cox 回归模型用于评估生存的候选预后因素。C-指数用于评估模型的判别能力。
中位随访 84 个月内,68 例患者出现 BCR,58 例患者出现疾病进展,其中仅 3 例出现局部进展,27 例患者因任何原因死亡,2 例患者死于 PCa。5 年 BCRFS、PFS、OS 和 CSS 率分别为 82.2%(HR 86.5%;VHR 70.0%)、90.0%(HR 94.3%;VHR 77.6%)、95.7%(HR,97.1%;VHR,91.8%)和 99.6%(HR,100%;VHR,98.0%)。在多变量分析中,调整了标准临床病理特征后,风险分类与 PFS 和 OS 均相关(p=0.0003 和 0.001)。添加风险分类可提高预测 BCRFS、PFS 和 OS 的模型的准确性。
虽然这种三联疗法的治疗效果似乎较好,但 VHR PCa 患者的肿瘤学预后明显差于 HR PCa 患者。NCCN 风险分类应纳入预后工具,以指导接受这种三联疗法的不利 PCa 患者的风险分层、治疗和随访。