Vaccine and Infectious Disease Division, Fred Hutchinson Cancer Research Center, Seattle, Washington, USA.
Department of Medicine, University of Washington, Seattle, Washington, USA.
JCI Insight. 2021 Jun 8;6(11):146743. doi: 10.1172/jci.insight.146743.
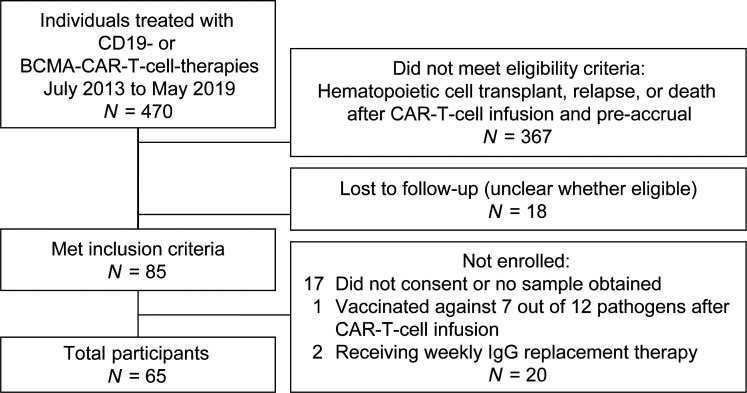
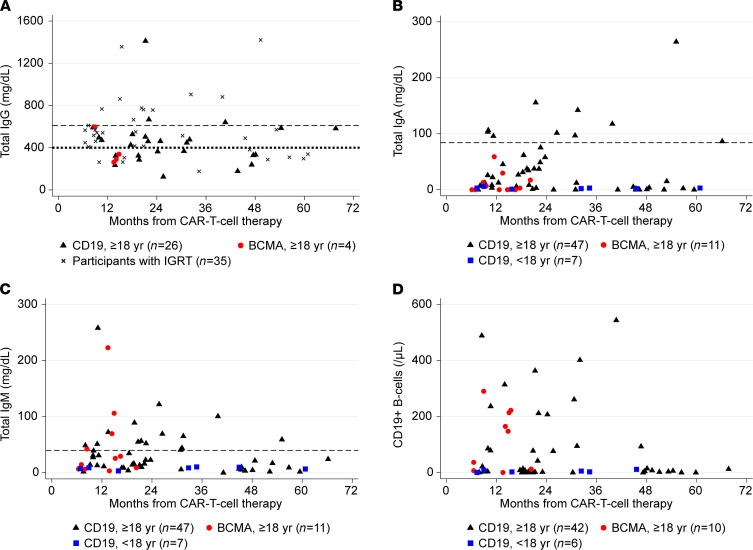
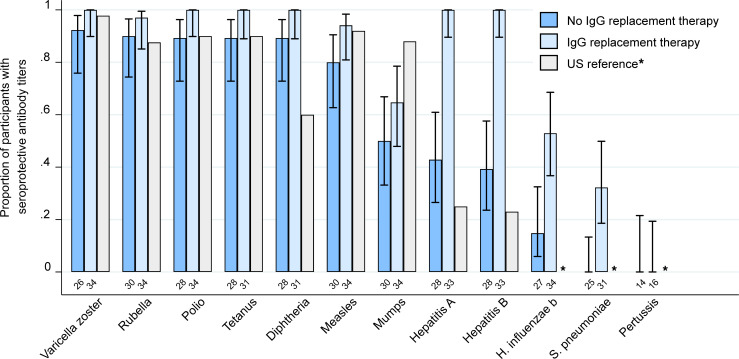
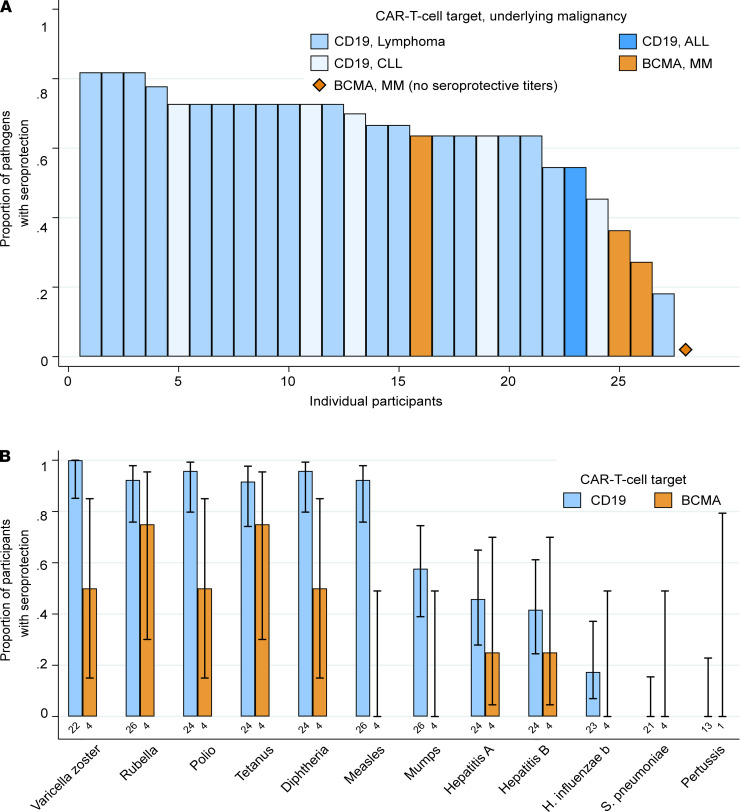
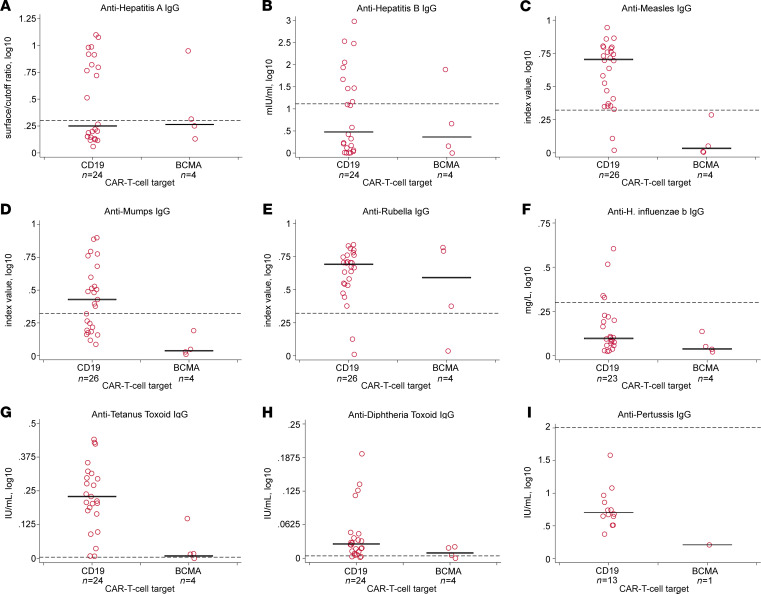
BACKGROUNDLittle is known about pathogen-specific humoral immunity after chimeric antigen receptor-modified T (CAR-T) cell therapy for B cell malignancies.METHODSWe conducted a prospective cross-sectional study of CD19-targeted or B cell maturation antigen-targeted (BCMA-targeted) CAR-T cell therapy recipients at least 6 months posttreatment and in remission. We measured pathogen-specific IgG against 12 vaccine-preventable infections and the number of viral and bacterial epitopes to which IgG was detected ("epitope hits") using a serological profiling assay. The primary outcome was the proportion of participants with IgG levels above a threshold correlated with seroprotection for vaccine-preventable infections.RESULTSWe enrolled 65 children and adults a median of 20 months after CD19- (n = 54) or BCMA- (n = 11) CAR-T cell therapy. Among 30 adults without IgG replacement therapy (IGRT) in the prior 16 weeks, 27 (90%) had hypogammaglobulinemia. These individuals had seroprotection to a median of 67% (IQR, 59%-73%) of tested infections. Proportions of participants with seroprotection per pathogen were comparable to population-based studies, but most individuals lacked seroprotection to specific pathogens. Compared with CD19-CAR-T cell recipients, BCMA-CAR-T cell recipients were half as likely to have seroprotection (prevalence ratio, 0.47; 95% CI, 0.18-1.25) and had fewer pathogen-specific epitope hits (mean difference, -90 epitope hits; 95% CI, -157 to -22).CONCLUSIONSeroprotection for vaccine-preventable infections in adult CD19-CAR-T cell recipients was comparable to the general population. BCMA-CAR-T cell recipients had fewer pathogen-specific antibodies. Deficits in both groups support the need for vaccine and immunoglobulin replacement therapy studies.FUNDINGSwiss National Science Foundation (Early Postdoc Mobility grant P2BSP3_188162), NIH/National Cancer Institute (NIH/NCI) (U01CA247548 and P01CA018029), NIH/NCI Cancer Center Support Grants (P30CA0087-48 and P30CA015704-44), American Society for Transplantation and Cellular Therapy, and Juno Therapeutics/BMS.
在接受嵌合抗原受体修饰 T(CAR-T)细胞疗法治疗 B 细胞恶性肿瘤后,人们对病原体特异性体液免疫知之甚少。
我们对至少在治疗后 6 个月且处于缓解期的靶向 CD19 或 B 细胞成熟抗原(BCMA-靶向)的 CAR-T 细胞治疗接受者进行了一项前瞻性的横断面研究。我们使用血清学分析检测了针对 12 种可通过疫苗预防的感染的病原体特异性 IgG 以及 IgG 检测到的病毒和细菌表位的数量(“表位命中”)。主要结局是 IgG 水平超过与可通过疫苗预防的感染相关的血清保护阈值的参与者比例。
我们纳入了中位数为 20 个月的 65 名儿童和成人,其中接受 CD19-(n = 54)或 BCMA-(n = 11)CAR-T 细胞治疗。在 16 周内未接受 IgG 替代治疗(IGRT)的 30 名成人中,有 27 名(90%)存在低丙种球蛋白血症。这些人对所测试感染的中位数为 67%(IQR,59%-73%)具有血清保护。每个病原体的血清保护率与基于人群的研究相当,但大多数个体缺乏针对特定病原体的血清保护。与 CD19-CAR-T 细胞受者相比,BCMA-CAR-T 细胞受者具有血清保护的可能性减半(患病率比,0.47;95%CI,0.18-1.25),且病原体特异性表位命中较少(平均差异,-90 个表位命中;95%CI,-157 至-22)。
在接受 CD19-CAR-T 细胞治疗的成年患者中,针对可通过疫苗预防的感染的血清保护率与一般人群相当。BCMA-CAR-T 细胞受者的病原体特异性抗体较少。两组的缺陷均支持疫苗和免疫球蛋白替代治疗研究的开展。
瑞士国家科学基金会(早期博士后流动资助 P2BSP3_188162)、美国国立卫生研究院/国家癌症研究所(NIH/NCI)(U01CA247548 和 P01CA018029)、NIH/NCI 癌症中心支持赠款(P30CA0087-48 和 P30CA015704-44)、美国移植和细胞治疗学会以及 Juno Therapeutics/BMS。