Cruz Da Silva Elisabete, Mercier Marie-Cécile, Etienne-Selloum Nelly, Dontenwill Monique, Choulier Laurence
CNRS, UMR 7021, Laboratoire de Bioimagerie et Pathologies, Faculté de Pharmacie, Université de Strasbourg, 67401 Illkirch, France.
Service de Pharmacie, Institut de Cancérologie Strasbourg Europe, 67200 Strasbourg, France.
Cancers (Basel). 2021 Apr 9;13(8):1795. doi: 10.3390/cancers13081795.
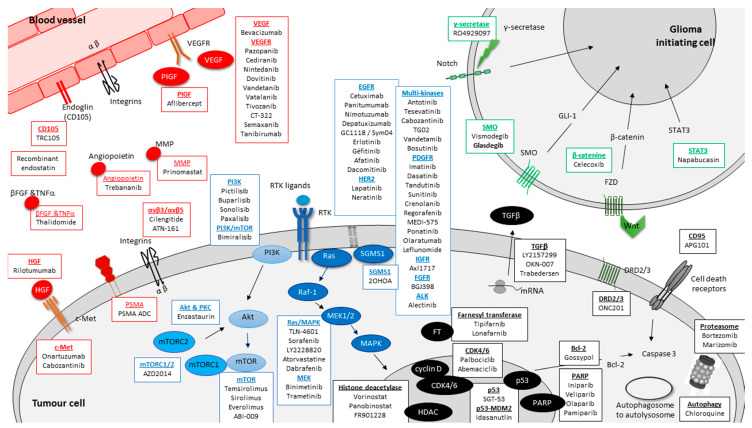
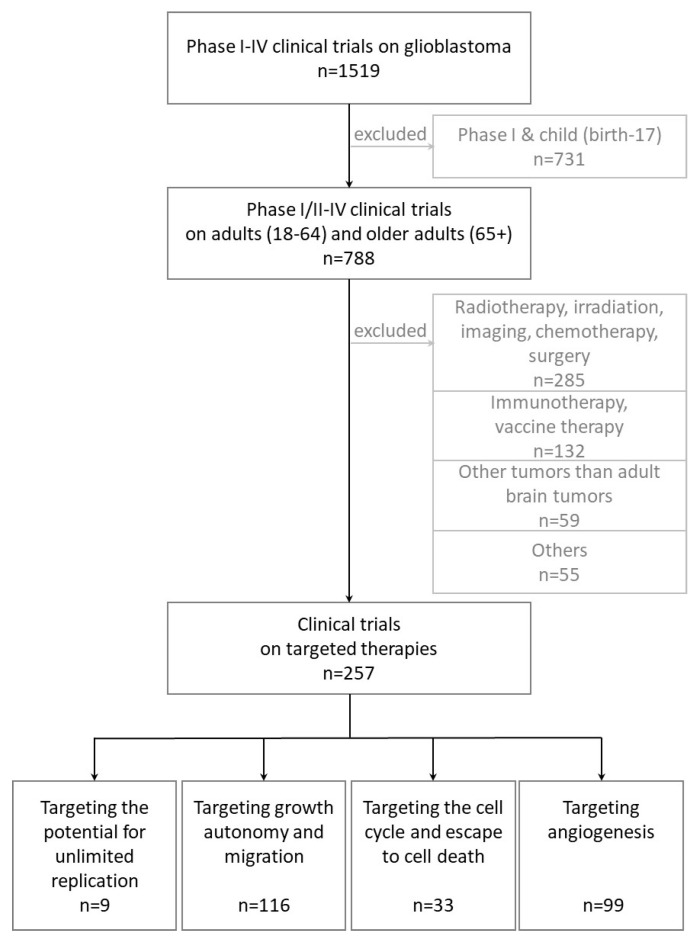
Glioblastoma (GBM), the most frequent and aggressive glial tumor, is currently treated as first line by the Stupp protocol, which combines, after surgery, radiotherapy and chemotherapy. For recurrent GBM, in absence of standard treatment or available clinical trials, various protocols including cytotoxic drugs and/or bevacizumab are currently applied. Despite these heavy treatments, the mean overall survival of patients is under 18 months. Many clinical studies are underway. Based on clinicaltrials.org and conducted up to 1 April 2020, this review lists, not only main, but all targeted therapies in phases II-IV of 257 clinical trials on adults with newly diagnosed or recurrent GBMs for the last twenty years. It does not involve targeted immunotherapies and therapies targeting tumor cell metabolism, that are well documented in other reviews. Without surprise, the most frequently reported drugs are those targeting (i) EGFR (40 clinical trials), and more generally tyrosine kinase receptors (85 clinical trials) and (ii) VEGF/VEGFR (75 clinical trials of which 53 involving bevacizumab). But many other targets and drugs are of interest. They are all listed and thoroughly described, on an one-on-one basis, in four sections related to targeting (i) GBM stem cells and stem cell pathways, (ii) the growth autonomy and migration, (iii) the cell cycle and the escape to cell death, (iv) and angiogenesis.
胶质母细胞瘤(GBM)是最常见且侵袭性最强的神经胶质瘤,目前按照Stupp方案进行一线治疗,该方案在手术后联合放疗和化疗。对于复发性GBM,在缺乏标准治疗方法或可用临床试验的情况下,目前应用了包括细胞毒性药物和/或贝伐单抗在内的各种方案。尽管进行了这些积极的治疗,患者的平均总生存期仍不到18个月。许多临床研究正在进行中。基于clinicaltrials.org并截至2020年4月1日,本综述列出了过去二十年来针对新诊断或复发性GBM成人患者的257项临床试验中II-IV期的所有靶向治疗方法,不仅包括主要的,还包括所有的。它不涉及靶向免疫疗法和针对肿瘤细胞代谢的疗法,这些在其他综述中有详细记载。不出所料,最常报道的药物是那些靶向(i)表皮生长因子受体(EGFR)(40项临床试验),更普遍地是酪氨酸激酶受体(85项临床试验)以及(ii)血管内皮生长因子/血管内皮生长因子受体(VEGF/VEGFR)(75项临床试验,其中53项涉及贝伐单抗)。但许多其他靶点和药物也值得关注。它们都在与靶向(i)GBM干细胞和干细胞途径、(ii)生长自主性和迁移、(iii)细胞周期和逃避细胞死亡、(iv)以及血管生成相关的四个部分中逐一列出并进行了详尽描述。