Secco Gianmarco, Salinaro Francesco, Bellazzi Carlo, La Salvia Marco, Delorenzo Marzia, Zattera Caterina, Barcella Bruno, Resta Flavia, Vezzoni Giulia, Bonzano Marco, Cappa Giovanni, Bruno Raffaele, Casagranda Ivo, Perlini Stefano
Emergency Medicine Unit and Emergency Medicine Postgraduate Training Program, Department of Internal Medicine, University of Pavia, IRCCS Policlinico San Matteo Foundation, 27100 Pavia, Italy.
Department of Electrical, Computer and Biomedical Engineering, University of Pavia, 27100 Pavia, Italy.
Diagnostics (Basel). 2021 Apr 23;11(5):761. doi: 10.3390/diagnostics11050761.
COVID-19 is an emerging infectious disease, that is heavily challenging health systems worldwide. Admission Arterial Blood Gas (ABG) and Lung Ultrasound (LUS) can be of great help in clinical decision making, especially during the current pandemic and the consequent overcrowding of the Emergency Department (ED). The aim of the study was to demonstrate the capability of alveolar-to-arterial oxygen difference (AaDO) in predicting the need for subsequent oxygen support and survival in patients with COVID-19 infection, especially in the presence of baseline normal PaO/FiO ratio (P/F) values.
A cohort of 223 swab-confirmed COVID-19 patients underwent clinical evaluation, blood tests, ABG and LUS in the ED. LUS score was derived from 12 ultrasound lung windows. AaDO was derived as AaDO = ((FiO) (Atmospheric pressure - HO pressure) - (PaCO/R)) - PaO. Endpoints were subsequent oxygen support need and survival.
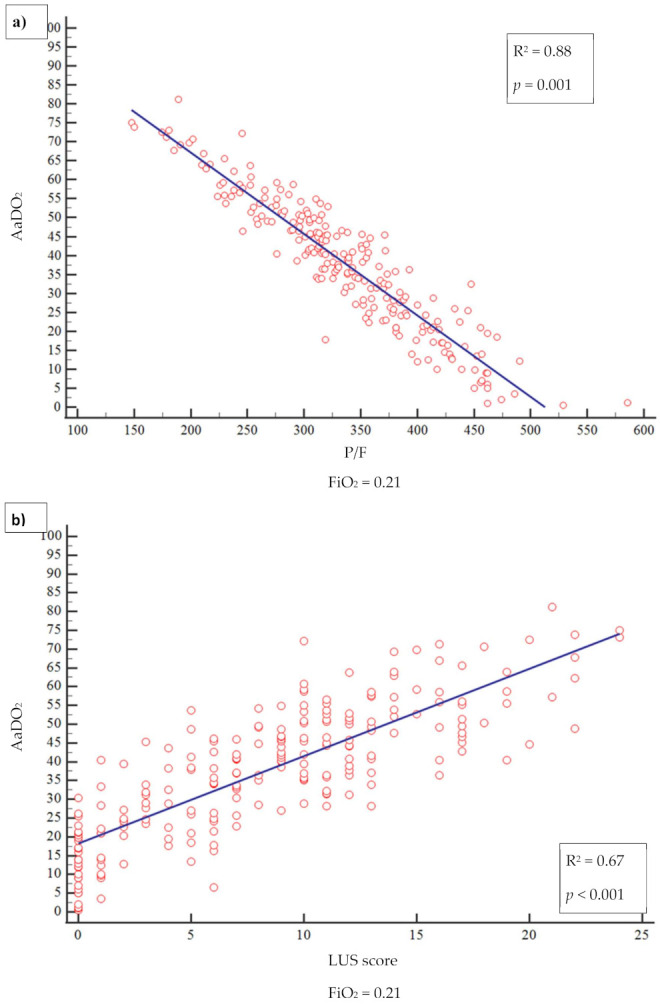
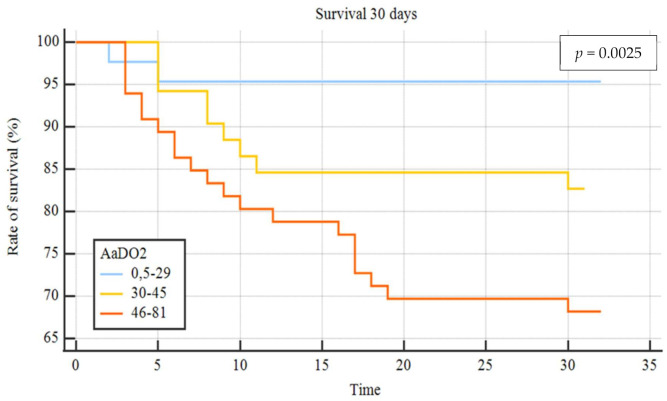
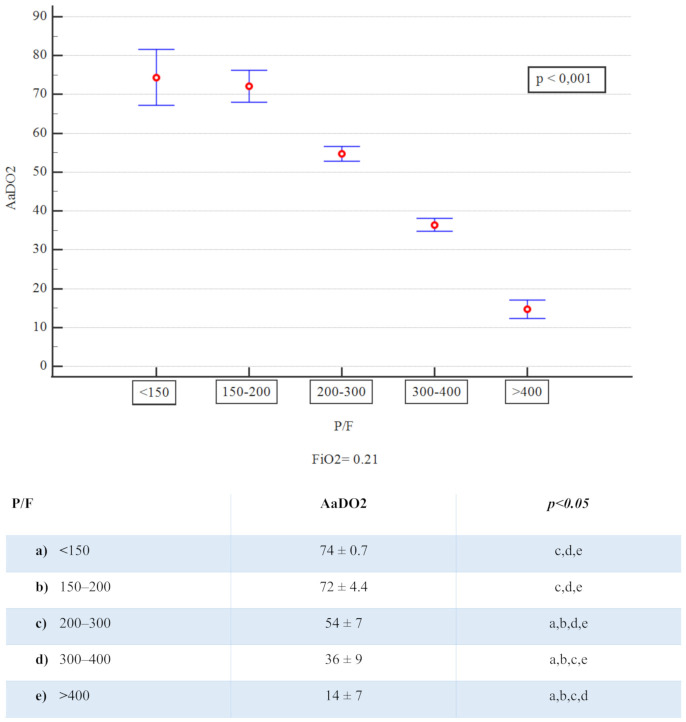
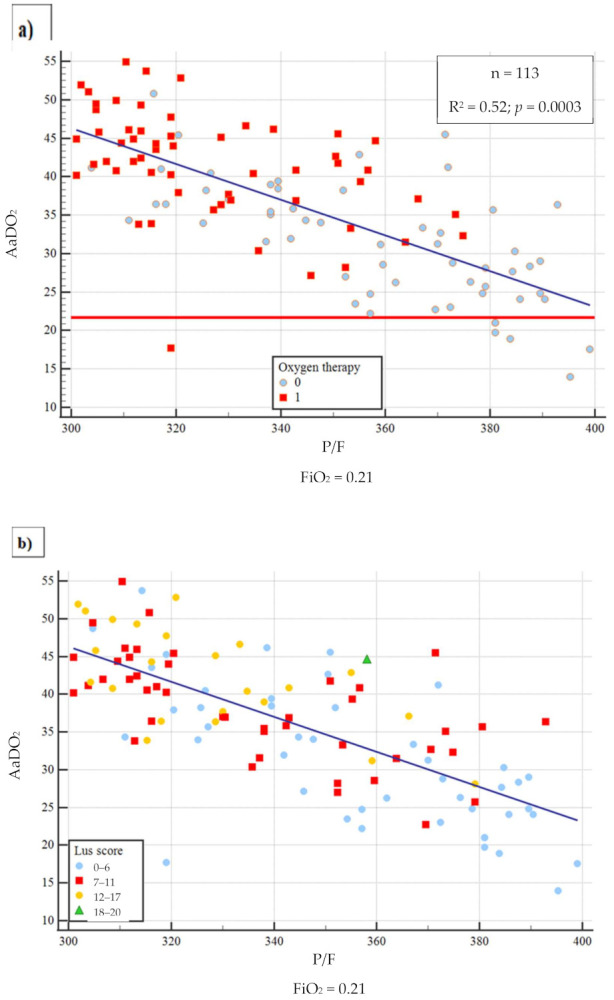
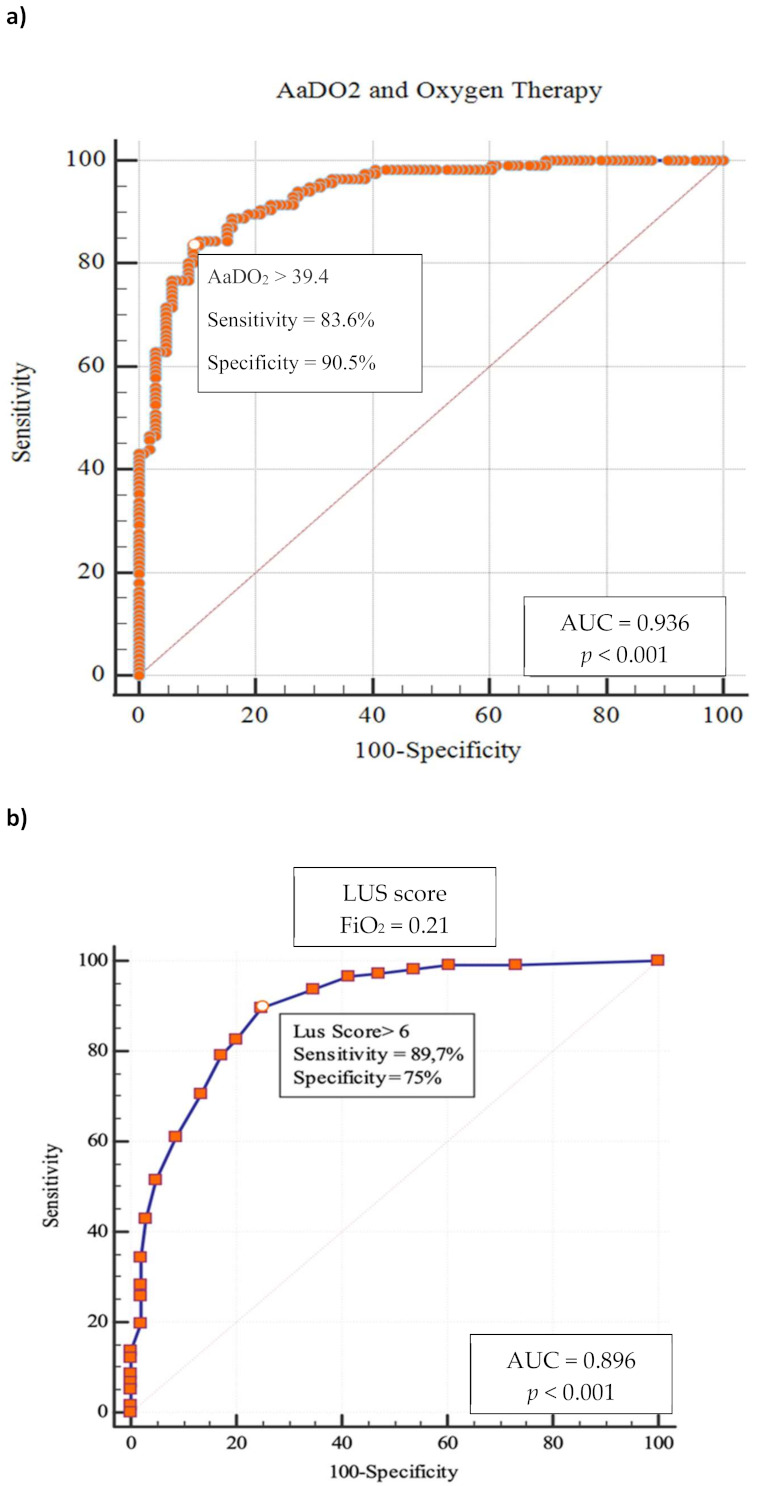
A close relationship between AaDO and P/F and between AaDO and LUS score was observed (R = 0.88 and R = 0.67, respectively; < 0.001 for both). In the subgroup of patients with P/F between 300 and 400, 94.7% ( = 107) had high AaDO values, and 51.4% ( = 55) received oxygen support, with 2 ICU admissions and 10 deaths. According to ROC analysis, AaDO > 39.4 had 83.6% sensitivity and 90.5% specificity (AUC 0.936; < 0.001) in predicting subsequent oxygen support, whereas a LUS score > 6 showed 89.7% sensitivity and 75.0% specificity (AUC 0.896; < 0.001). Kaplan-Meier curves showed different mortality in the AaDO subgroups ( = 0.0025).
LUS and AaDO are easy and effective tools, which allow bedside risk stratification in patients with COVID-19, especially when P/F values, signs, and symptoms are not indicative of severe lung dysfunction.
新型冠状病毒肺炎(COVID-19)是一种新出现的传染病,给全球卫生系统带来了巨大挑战。入院时动脉血气分析(ABG)和肺部超声(LUS)对临床决策有很大帮助,尤其是在当前疫情期间以及急诊科(ED)因此出现过度拥挤的情况下。本研究的目的是证明肺泡-动脉氧分压差(AaDO)在预测COVID-19感染患者后续是否需要氧疗及生存情况方面的能力,特别是在基线时动脉血氧分压/吸入氧分数值(P/F)正常的情况下。
对223例经拭子检测确诊的COVID-19患者在急诊科进行了临床评估、血液检查、ABG和LUS检查。LUS评分来自12个超声肺部检查区域。AaDO的计算方法为AaDO = [(FiO)(大气压 - 水蒸气压力) - (PaCO₂/呼吸商)] - PaO₂。观察终点为后续是否需要氧疗及生存情况。
观察到AaDO与P/F以及AaDO与LUS评分之间存在密切关系(相关系数R分别为0.88和0.67;两者均P < 0.001)。在P/F为300至400的患者亚组中,94.7%(n = 107)的AaDO值较高,51.4%(n = 55)接受了氧疗,其中2例入住重症监护病房(ICU),10例死亡。根据ROC分析,AaDO > 39.4在预测后续是否需要氧疗方面的敏感度为83.6%,特异度为90.5%(曲线下面积[AUC]为0.936;P < 0.001),而LUS评分> 6时的敏感度为89.7%,特异度为75.0%(AUC为0.896;P < 0.001)。Kaplan-Meier曲线显示AaDO亚组的死亡率不同(P = 0.0025)。
LUS和AaDO是简单有效的工具,可对COVID-19患者进行床旁风险分层,尤其是当P/F值、体征和症状不能提示严重肺功能障碍时。