Contreras Yametti Gloria Paz, Ostrow Talia H, Jasinski Sylwia, Raetz Elizabeth A, Carroll William L, Evensen Nikki A
Division of Pediatric Hematology Oncology, NYU Langone Health, New York, NY 10016, USA.
Department of Pediatric and Pathology, Perlmutter Cancer Center, NYU Langone Health, Smillow 1211, 560 First Avenue, New York, NY 10016, USA.
Cancers (Basel). 2021 Apr 13;13(8):1847. doi: 10.3390/cancers13081847.
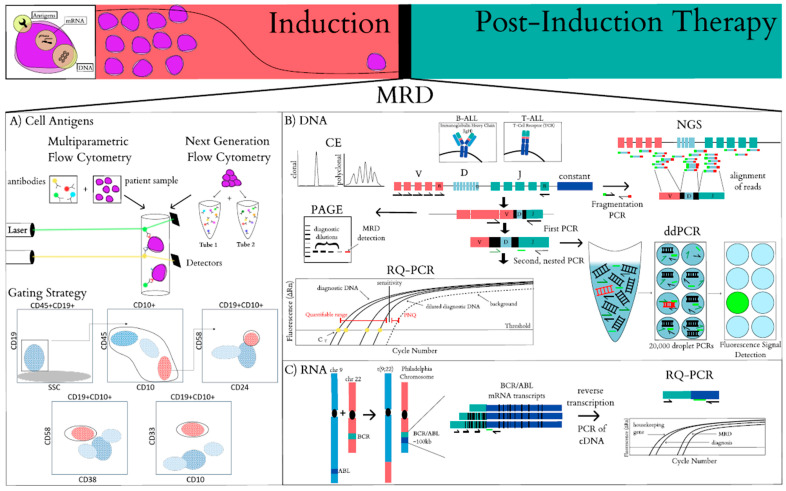
Acute lymphoblastic leukemia (ALL) is the most common pediatric cancer and advances in its clinical and laboratory biology have grown exponentially over the last few decades. Treatment outcome has improved steadily with over 90% of patients surviving 5 years from initial diagnosis. This success can be attributed in part to the development of a risk stratification approach to identify those subsets of patients with an outstanding outcome that might qualify for a reduction in therapy associated with fewer short and long term side effects. Likewise, recognition of patients with an inferior prognosis allows for augmentation of therapy, which has been shown to improve outcome. Among the clinical and biological variables known to impact prognosis, the kinetics of the reduction in tumor burden during initial therapy has emerged as the most important prognostic variable. Specifically, various methods have been used to detect minimal residual disease (MRD) with flow cytometric and molecular detection of antigen receptor gene rearrangements being the most common. However, many questions remain as to the optimal timing of these assays, their sensitivity, integration with other variables and role in treatment allocation of various ALL subgroups. Importantly, the emergence of next generation sequencing assays is likely to broaden the use of these assays to track disease evolution. This review will discuss the biological basis for utilizing MRD in risk assessment, the technical approaches and limitations of MRD detection and its emerging applications.
急性淋巴细胞白血病(ALL)是最常见的儿童癌症,在过去几十年中,其临床和实验室生物学方面的进展呈指数级增长。治疗结果稳步改善,超过90%的患者从初次诊断起存活5年。这一成功部分归因于风险分层方法的发展,该方法用于识别那些可能有出色预后结果的患者亚组,这些患者可能有资格减少治疗,且短期和长期副作用较少。同样,识别预后较差的患者有助于加强治疗,这已被证明可改善治疗结果。在已知影响预后的临床和生物学变量中,初始治疗期间肿瘤负荷降低的动力学已成为最重要的预后变量。具体而言,已使用多种方法检测微小残留病(MRD),其中流式细胞术和抗原受体基因重排的分子检测最为常见。然而,关于这些检测的最佳时机、其敏感性、与其他变量的整合以及在各种ALL亚组治疗分配中的作用,仍存在许多问题。重要的是,新一代测序检测的出现可能会扩大这些检测在跟踪疾病演变方面的应用。本综述将讨论在风险评估中利用MRD的生物学基础、MRD检测的技术方法和局限性及其新兴应用。