Liang Zhe, Chen Qi, Wei Ruiqi, Ma Chenyao, Zhang Xuehui, Chen Xue, Fang Fang, Zhao Quanming
Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, Beijing, China.
Department of Sleep Medical Center, Beijing Anzhen Hospital, Capital Medical University, Beijing, China.
Front Pharmacol. 2021 Apr 14;12:648244. doi: 10.3389/fphar.2021.648244. eCollection 2021.
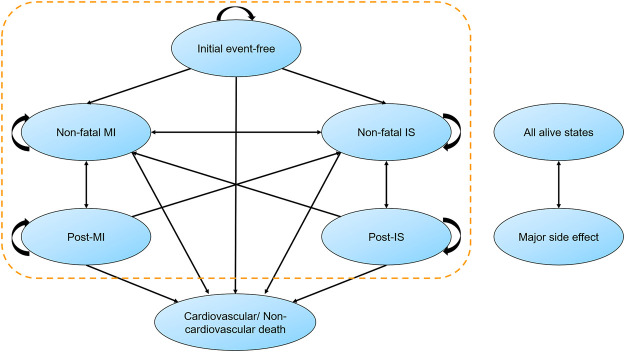
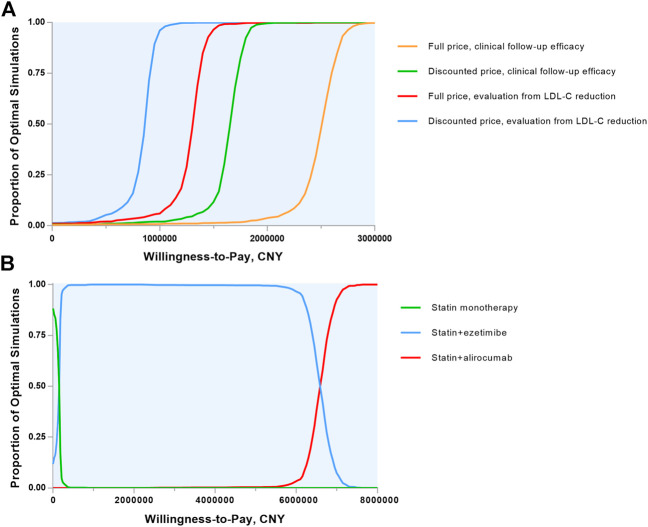
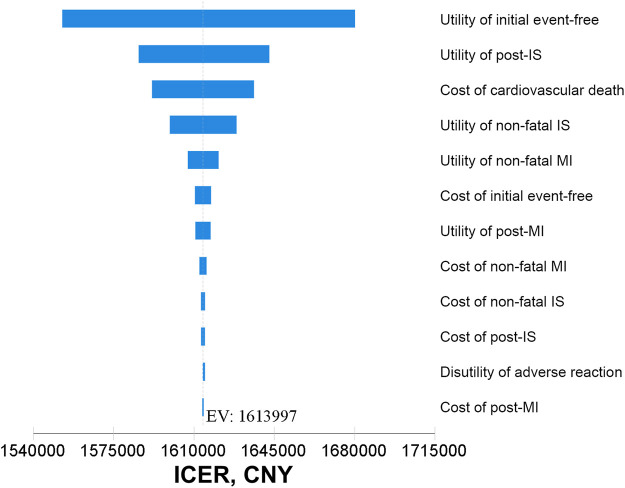
Proprotein convertase subtilisin/kexin type 9 inhibitor alirocumab reduce ischemic events; however, the cost-effectiveness remains uncertain. This study sought to evaluate its economic value in patients with myocardial infarction (MI) from the Chinese healthcare perspective. A state-transition Markov model was developed to determine the cost-effectiveness of alirocumab for preventing recurrent MI, ischemic stroke and death. Preventative effect of the therapy was gathered from ODYSSEY OUTCOMES trial and absolute reduction of low-density lipoprotein cholesterol (LDL-C) in ODYSSEY EAST trial, respectively. The primary outcome was the incremental cost-effectiveness ratio (ICER), defined as incremental cost per quality-adjusted life-year (QALY) gained. Compared with statin monotherapy, the ICER of alirocumab therapy at its present discounted price [34,355 Chinese yuan (CNY) annually, 33% rebate] based on clinical follow-up efficacy was 1,613,997 CNY per QALY gained. A willingness-to-pay threshold of 212,676 CNY per QALY would be achieved when the annual cost of alirocumab was reduced by 88% from the full official price to 6071 CNY. The therapeutic effect evaluation estimated by the magnitude of LDL-C reduction was superior to the results of clinical follow-up, but this medication was still far from cost-effective. Multiple vulnerable subgroup analyses demonstrated that the ICER for patients with polyvascular disease in 3 vascular beds was 111,750 CNY per QALY gained. Alirocumab is not cost-effective in general MI population based on current discounted price. High long-term costs of alirocumab may be offset by health benefit in patients with polyvascular disease (3 beds).
前蛋白转化酶枯草溶菌素/凯新9型抑制剂阿利西尤单抗可减少缺血事件;然而,其成本效益仍不确定。本研究旨在从中国医疗保健角度评估其在心肌梗死(MI)患者中的经济价值。建立了一个状态转换马尔可夫模型,以确定阿利西尤单抗预防复发性心肌梗死、缺血性中风和死亡的成本效益。该疗法的预防效果分别来自ODYSSEY OUTCOMES试验和ODYSSEY EAST试验中低密度脂蛋白胆固醇(LDL-C)的绝对降低量。主要结局是增量成本效益比(ICER),定义为每获得一个质量调整生命年(QALY)的增量成本。与他汀类药物单药治疗相比,基于临床随访疗效,阿利西尤单抗治疗目前的贴现价格(每年34355元人民币,33%折扣)的ICER为每获得一个QALY 1613997元人民币。当阿利西尤单抗的年度成本从全价降低88%至6071元人民币时,将达到每QALY 212676元人民币的支付意愿阈值。通过LDL-C降低幅度估计的治疗效果评估优于临床随访结果,但这种药物仍远未达到成本效益。多项脆弱亚组分析表明,在3个血管床患有多血管疾病的患者中,ICER为每获得一个QALY 111750元人民币。基于目前的贴现价格,阿利西尤单抗在一般心肌梗死人群中不具有成本效益。阿利西尤单抗高昂的长期成本可能会被多血管疾病(3个血管床)患者的健康益处所抵消。