Kim Min Young, Brennan Daniel C
Department of Internal Medicine, Johns Hopkins School of Medicine, Baltimore, MD, United States.
Front Pharmacol. 2021 Apr 15;12:651222. doi: 10.3389/fphar.2021.651222. eCollection 2021.
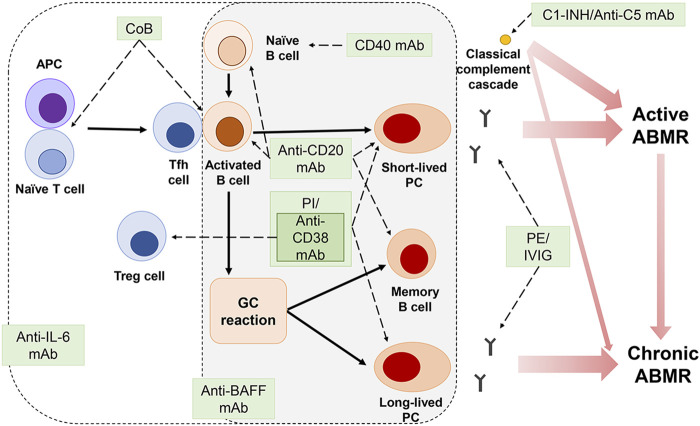
Remarkable advances have been made in the pathophysiology, diagnosis, and treatment of antibody-mediated rejection (ABMR) over the past decades, leading to improved graft outcomes. However, long-term failure is still high and effective treatment for chronic ABMR, an important cause of graft failure, has not yet been identified. Chronic ABMR has a relatively different phenotype from active ABMR and is a slowly progressive disease in which graft injury is mainly caused by donor specific antibodies (DSA). Since most trials of current immunosuppressive therapies for rejection have focused on active ABMR, treatment strategies based on those data might be less effective in chronic ABMR. A better understanding of chronic ABMR may serve as a bridge in establishing treatment strategies to improve graft outcomes. In this in-depth review, we focus on the pathophysiology and characteristics of chronic ABMR along with the newly revised Banff criteria in 2017. In addition, in terms of chronic ABMR, we identify the reasons for the resistance of current immunosuppressive therapies and look at ongoing research that could play a role in setting better treatment strategies in the future. Finally, we review non-invasive biomarkers as tools to monitor for rejection.
在过去几十年中,抗体介导的排斥反应(ABMR)的病理生理学、诊断和治疗取得了显著进展,从而改善了移植物的预后。然而,长期失败率仍然很高,对于作为移植物失败重要原因的慢性ABMR,尚未确定有效的治疗方法。慢性ABMR与活动性ABMR具有相对不同的表型,是一种缓慢进展的疾病,其中移植物损伤主要由供体特异性抗体(DSA)引起。由于目前大多数针对排斥反应的免疫抑制疗法试验都集中在活动性ABMR上,基于这些数据的治疗策略在慢性ABMR中可能效果较差。更好地了解慢性ABMR可能有助于建立改善移植物预后的治疗策略。在这篇深入综述中,我们重点关注慢性ABMR的病理生理学和特征以及2017年新修订的班夫标准。此外,就慢性ABMR而言,我们确定了当前免疫抑制疗法耐药的原因,并探讨了可能在未来制定更好治疗策略中发挥作用的正在进行的研究。最后,我们回顾了作为监测排斥反应工具的非侵入性生物标志物。