Zaine Hind, Vandendorpe Benjamin, Bataille Benoit, Lacornerie Thomas, Wallet Jennifer, Mirabel Xavier, Lartigau Eric, Pasquier David
Academic Department of Radiation Oncology, Centre Oscar Lambret, Lille, France.
Department of Medical Physics, Centre O. Lambret, Lille, France.
Front Oncol. 2021 Apr 15;11:669261. doi: 10.3389/fonc.2021.669261. eCollection 2021.
Salvage radiotherapy is the only curative treatment for biochemical progression after radical prostatectomy. Macroscopic recurrence may be found in the prostatic bed. The purpose of our study is to evaluate the effectiveness of salvage radiotherapy of the prostate bed with a boost to the area of the macroscopic recurrence.
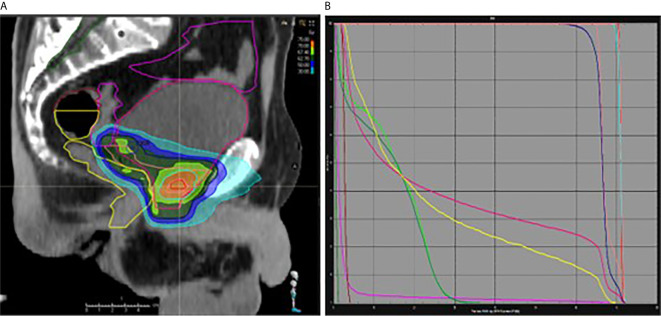
From January 2005 to January 2020, 89 patients with macroscopic recurrence in the prostatectomy bed were treated with salvage radiotherapy +/- hormone therapy. The average PSA level prior to radiotherapy was 1.1 ng/mL (SD: 1.6). At the time of biochemical progression, 96% of the patients had a MRI that revealed the macroscopic recurrence, and 58% had an additional choline PET scan. 67.4% of the patients got a boost to the macroscopic nodule, while 32.5% of the patients only underwent radiotherapy of the prostate bed without a boost. The median total dose of radiotherapy was 70 Gy (Min.: 60 - Max.: 74). The most commonly-used regimen was radiotherapy of the prostatectomy bed with a concomitant boost. 48% of the patients were concomitantly treated with hormone therapy.
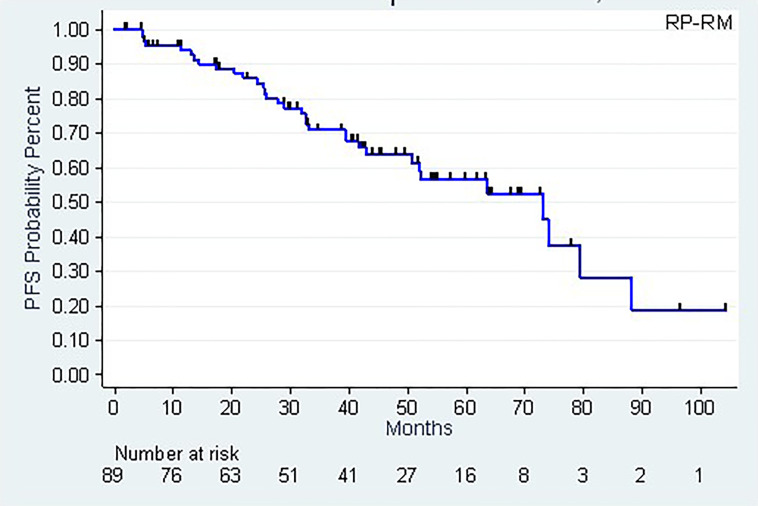
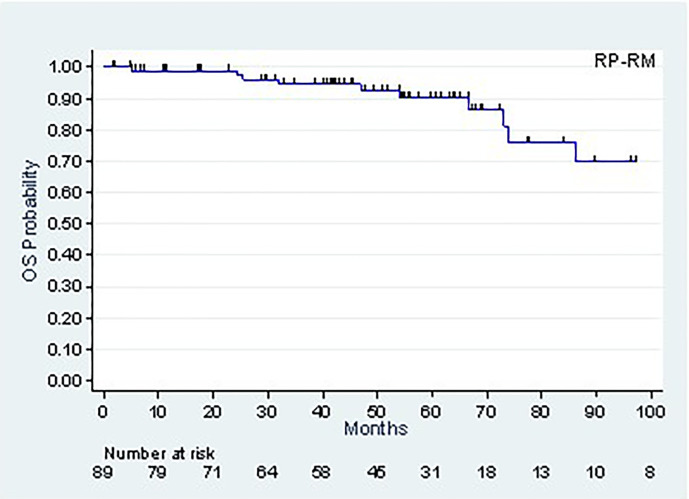
After a median follow-up of 53.7 months, 77 patients were alive and 12 had died, of which 4 following metastatic progression. The 5-year and 8-year survival rates (CI95%) are, respectively, 90.2% (78.9-95.6%) and 69.8% (46.4-84.4%). The 5-year biochemical progression-free survival rate (CI95%) is 50.8% (36.7-63.3). Metastatic recurrence occurred in 11.2% of the patients. We did not find any statistically significant impact from the various known prognostic factors for biochemical progression-free survival. No toxicity with a grade of > or = to 3 was found.
Our series is one of the largest published to date. Salvage radiotherapy has its place in the management of patients with biochemical progression with local recurrence in the prostate bed, with an acceptable toxicity profile. The interest of the boost is to be evaluated in prospective trials.
挽救性放疗是根治性前列腺切除术后生化进展的唯一治愈性治疗方法。肉眼可见的复发可能出现在前列腺床。本研究的目的是评估对前列腺床进行挽救性放疗并对肉眼可见复发区域进行加量照射的有效性。
2005年1月至2020年1月,89例前列腺切除床出现肉眼可见复发的患者接受了挽救性放疗±激素治疗。放疗前的平均前列腺特异抗原(PSA)水平为1.1 ng/mL(标准差:1.6)。在生化进展时,96%的患者进行了磁共振成像(MRI)检查,显示有肉眼可见的复发,58%的患者还进行了胆碱正电子发射断层扫描(PET)。67.4%的患者对肉眼可见结节进行了加量照射,而32.5%的患者仅接受了前列腺床放疗而未进行加量照射。放疗的中位总剂量为70 Gy(最小值:60 - 最大值:74)。最常用的方案是对前列腺切除床进行放疗并同时进行加量照射。48%的患者同时接受了激素治疗。
中位随访53.7个月后,77例患者存活,12例死亡,其中4例死于转移进展。5年和8年生存率(95%置信区间)分别为90.2%(78.9 - 95.6%)和69.8%(46.4 - 84.4%)。5年无生化进展生存率(95%置信区间)为50.8%(36.7 - 63.3)。11.2%的患者出现转移复发。我们未发现任何已知的生化无进展生存预后因素有统计学意义的影响。未发现3级及以上毒性反应。
我们的系列研究是迄今为止已发表的最大规模研究之一。挽救性放疗在前列腺床局部复发的生化进展患者的治疗中占有一席之地,其毒性可接受。加量照射的益处有待在前瞻性试验中评估。