Whittall Street Clinic, University Hospitals Birmingham NHS Trust, Birmingham, United Kingdom.
PLoS One. 2021 May 3;16(5):e0250883. doi: 10.1371/journal.pone.0250883. eCollection 2021.
To review the effect of different intramuscular injection (IMI) techniques on injection associated pain, in adults.
The review protocol was registered on PROSPERO (CRD42019136097). MEDLINE, EMBASE, British Nursing Index and CINAHL were searched up to June 2020. Included studies were appraised and a meta-analysis, where appropriate, was conducted with a random effects model and test for heterogeneity. Standardised mean difference (SMD) with a 95% confidence interval in reported injection pain (intervention cf. control) was reported.
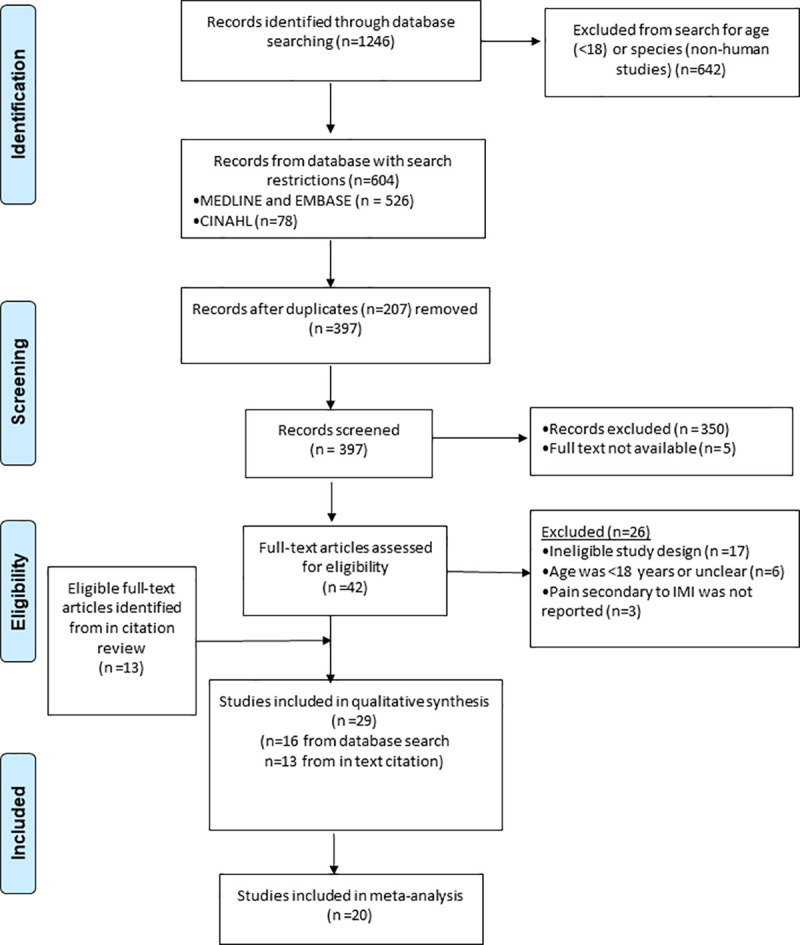
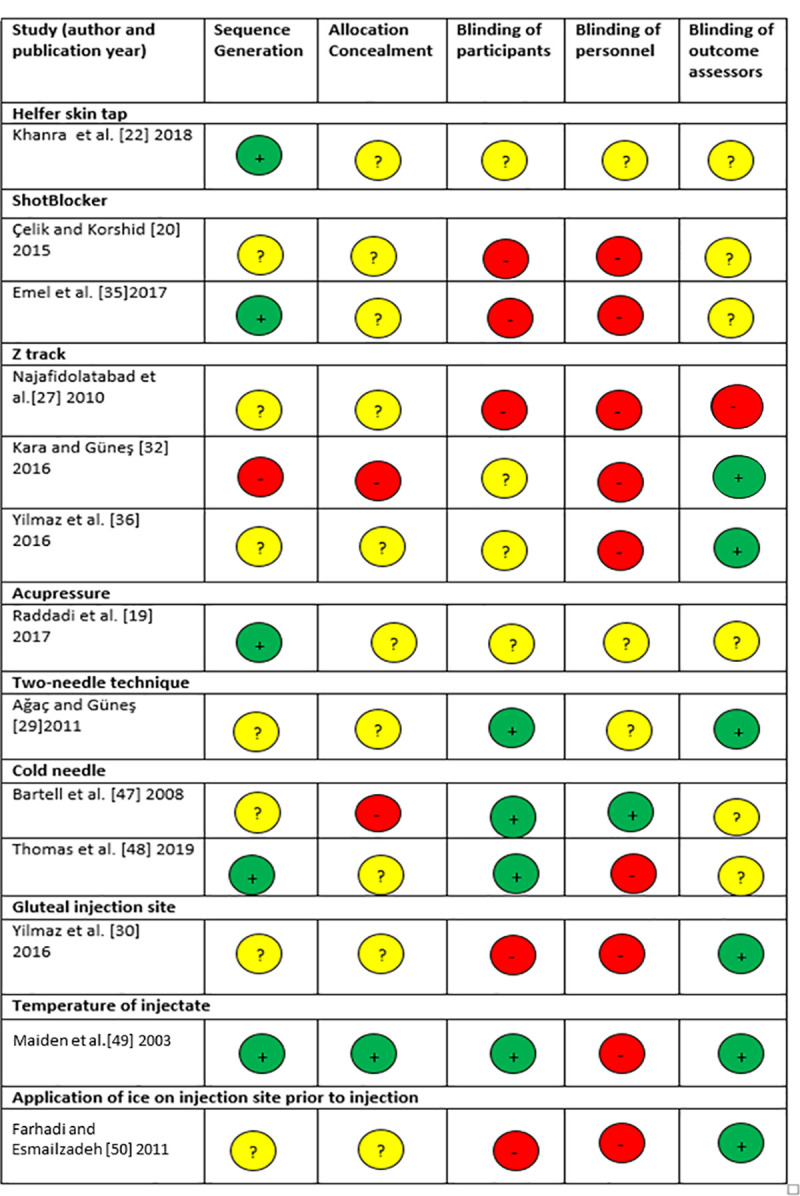
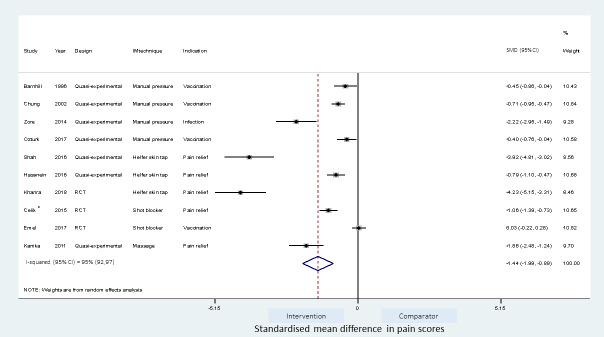
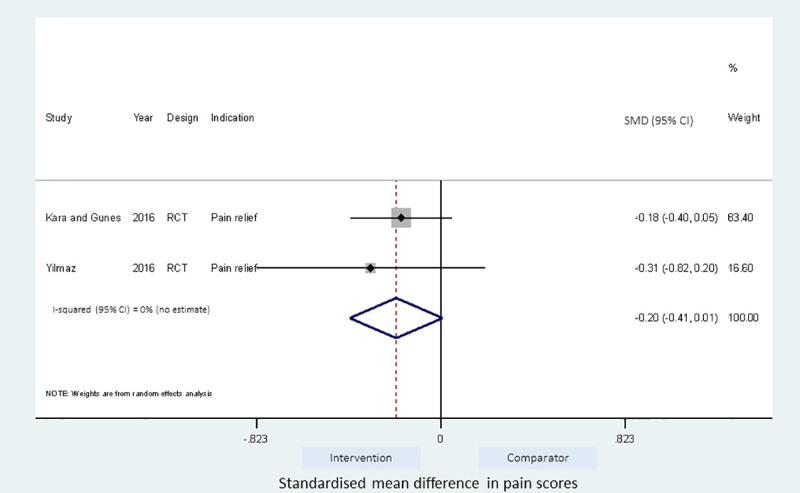
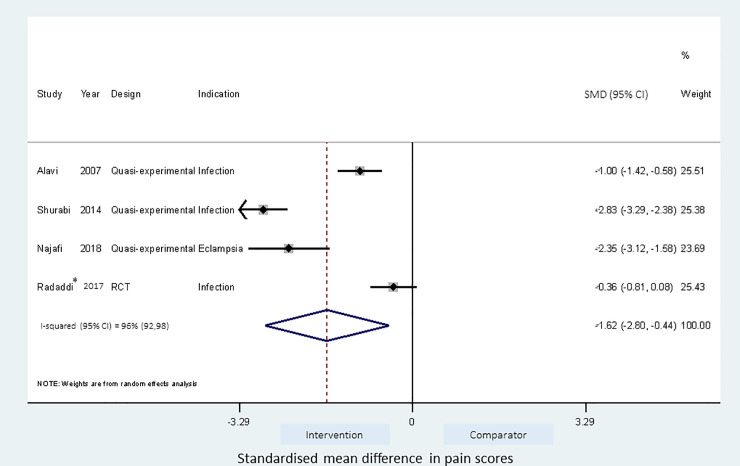
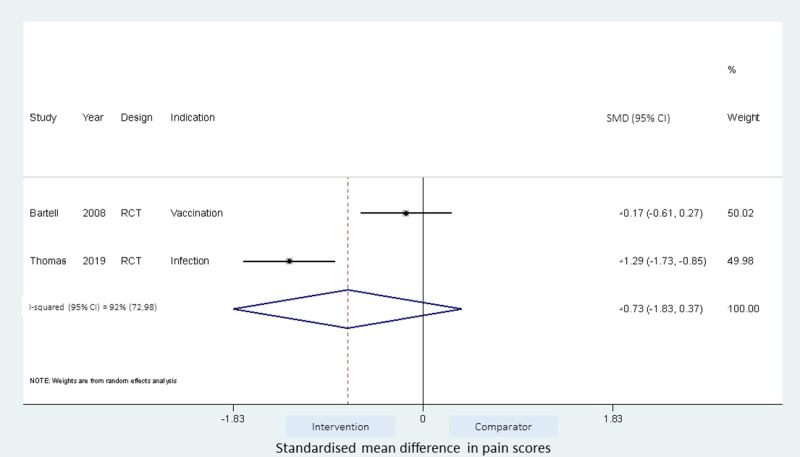
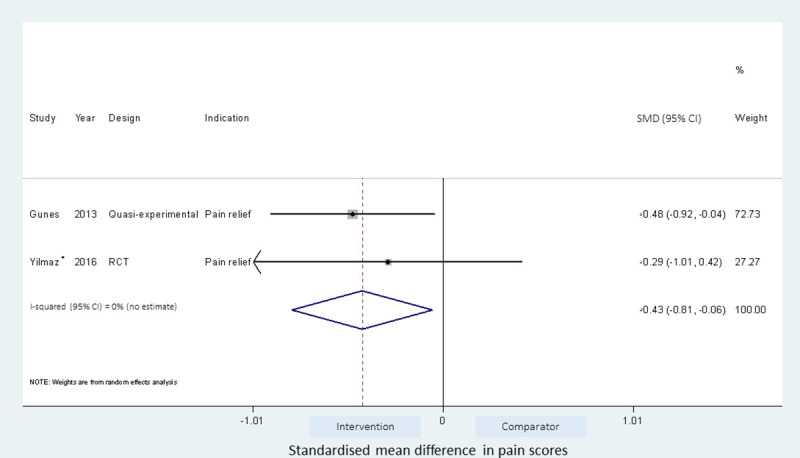
29 studies were included in the systematic review and 20 studies in the meta-analysis. 13 IMI techniques were identified. 10 studies applied local pressure to the injection site. Of these, applying manual pressure (4 studies, SMD = -0.85[-1.36,-0.33]) and Helfer (rhythmic) tapping (3 studies, SMD = -2.95[-5.51,-0.39]) to the injection site reduced injection pain, whereas the use of a plastic device to apply local pressure to the skin (ShotBlocker) did not significantly reduce pain (2 studies, SMD = -0.51[-1.58,0.56]). Acupressure techniques which mostly involved applying sustained pressure followed by intermittent pressure (tapping) to acupressure points local to the injection site reduced pain (4 studies: SMD = -1.62[-2.80,-0.44]), as did injections to the ventrogluteal site compared to the dorsogluteal site (2 studies, SMD = -0.43[-0.81,-0.06]). There was insufficient evidence on the benefits of the 'Z track technique' (2 studies, SMD = -0.20[-0.41,0.01]) and the cold needle technique (2 studies, SMD = -0.73[-1.83,0.37]) on injection pain. The effect of changing the needle after drawing up the injectate on injection pain was conflicting and warming the injectate did not reduce pain. Limitations included considerable heterogeneity, poor reporting of randomisation, and possible bias in outcome measures from unblinding of assessors or participants.
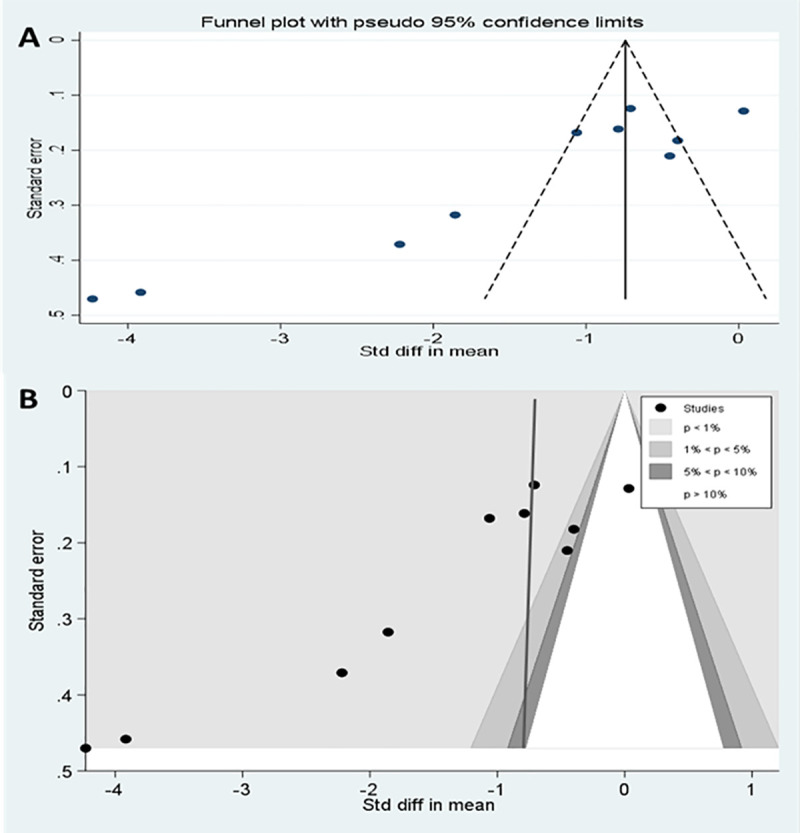
Manual pressure or rhythmic tapping over the injection site and applying local pressure around the injection site reduced IMI pain. However, there was very high unexplained heterogeneity between studies and risk of significant bias within small studies.
综述不同肌内注射(IMI)技术对成人注射相关疼痛的影响。
综述方案在 PROSPERO(CRD42019136097)上进行了注册。检索了 MEDLINE、EMBASE、英国护理索引和 CINAHL,检索时间截至 2020 年 6 月。对纳入的研究进行评估,并根据需要采用随机效应模型和异质性检验进行荟萃分析。报告报告的注射疼痛(干预与对照)的标准化均数差(SMD)和 95%置信区间。
系统评价纳入了 29 项研究,荟萃分析纳入了 20 项研究。确定了 13 种 IMI 技术。10 项研究对注射部位施加局部压力。其中,对注射部位施加手动压力(4 项研究,SMD=-0.85[-1.36,-0.33])和 Helfer(有节奏)叩诊(3 项研究,SMD=-2.95[-5.51,-0.39])可减轻注射疼痛,而使用塑料装置对皮肤施加局部压力(ShotBlocker)不能显著减轻疼痛(2 项研究,SMD=-0.51[-1.58,0.56])。主要涉及对注射部位附近的穴位施加持续压力然后施加间歇性压力(叩诊)的穴位按压技术可减轻疼痛(4 项研究:SMD=-1.62[-2.80,-0.44]),与臀肌外侧注射部位相比,臀肌上部注射部位的疼痛减轻(2 项研究,SMD=-0.43[-0.81,-0.06])。关于“Z 轨道技术”(2 项研究,SMD=-0.20[-0.41,0.01])和“冷针技术”(2 项研究,SMD=-0.73[-1.83,0.37])对注射疼痛的益处的证据不足。在抽取注射剂后更换针头对注射疼痛的影响存在争议,加热注射剂并不能减轻疼痛。局限性包括异质性较大、随机分组报告不佳以及评估者或参与者的结果测量存在无法掩盖的偏倚的风险。
在注射部位施加手动压力或有节奏的叩诊,以及在注射部位周围施加局部压力可减轻 IMI 疼痛。然而,研究之间存在非常高的无法解释的异质性,并且在小研究中存在显著偏倚的风险。