Division of Pediatric Cardiology, Department of Pediatrics, Leiden University Medical Center, Leiden, Netherlands.
Division of Pediatric Cardiology, Department of Pediatrics, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands.
Eur J Cardiothorac Surg. 2021 May 8;59(5):968-977. doi: 10.1093/ejcts/ezab006.
The objective of this study was to assess our 43-year experience with arterial switch operation (ASO) for transposition of the great arteries (TGA) by analysing cardiac outcome measures (hospital and late mortality, reoperations and catheter interventions, significant coronary artery obstruction) and to identify risk factors for reoperation and catheter interventions.
A total of 490 patients who underwent ASO for TGA from 1977 to 2020 were included in this retrospective, single-centre study. Data on reoperation and catheter intervention of hospital survivors were estimated by the Kaplan-Meier method and compared using a long-rank test. Risk factors for reoperation and/or catheter intervention were assessed by multivariate Cox regression analysis.
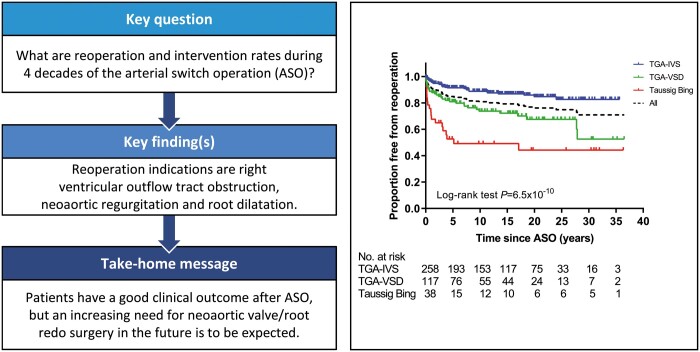
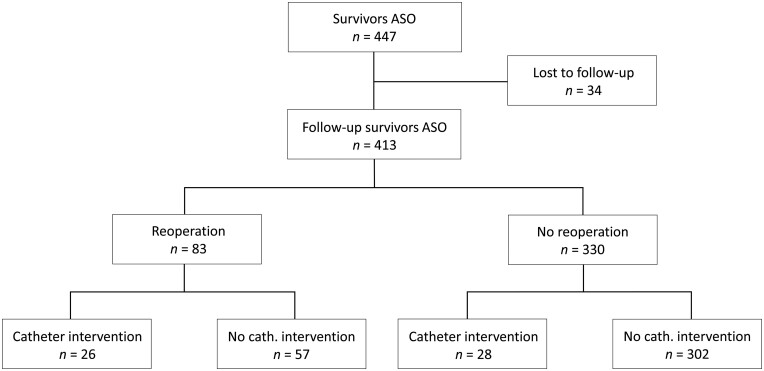
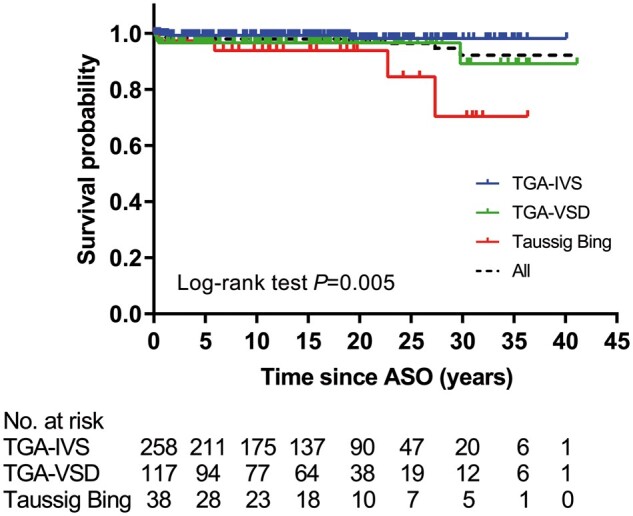
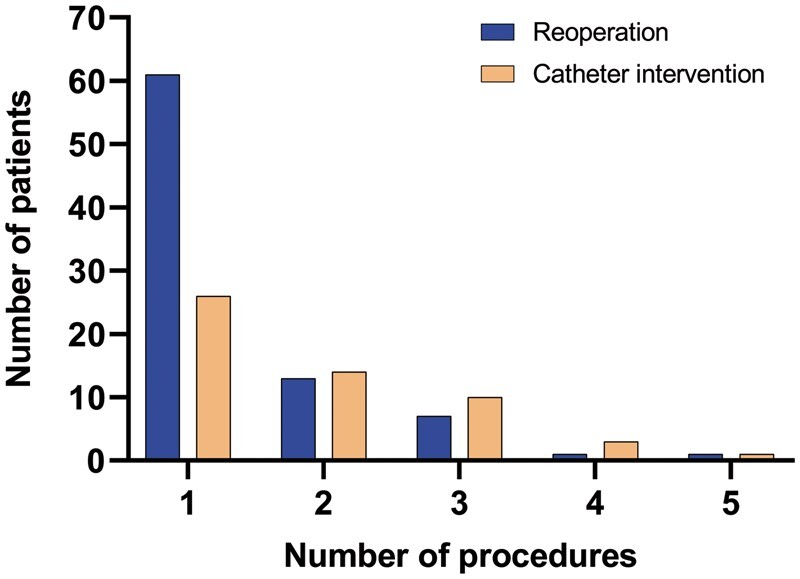
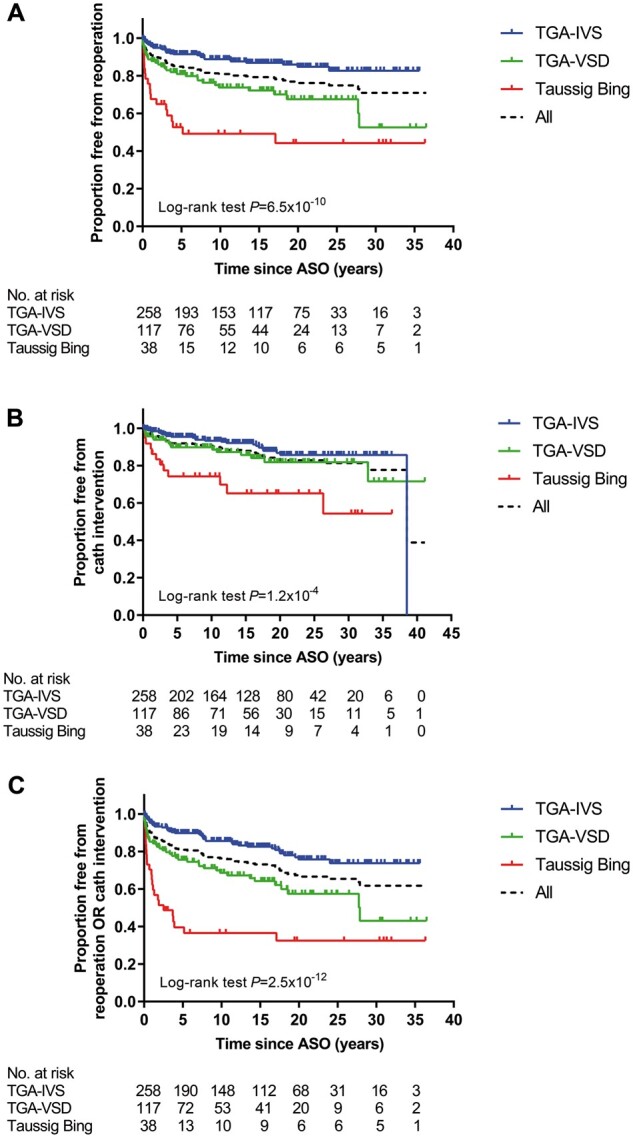
Hospital mortality occurred in 43 patients (8.8%), late death in 12 patients (2.9%) and 43 patients were lost to follow-up. Median follow-up time of 413 hospital survivors was 15.6 (interquartile range 7.0-22.4) years. Reoperations were performed in 83 patients (117 reoperations). Neoaortic valve regurgitation with root dilatation was the second most common indication for reoperation (15/83 patients, 18.1%) after right ventricular outflow tract obstruction (50/83 patients, 60.2%). Risk factors for any reoperation on multivariable analysis were: TGA morphological subtype [TGA with ventricular septal defect: hazard ratio (HR) = 1.99, 95% confidence interval (CI) 1.18-3.36; P = 0.010 and Taussig-Bing: HR = 2.17, 95% CI 1.02-4.64; P = 0.045], aortic arch repair associated with ASO (HR = 3.03, 95% CI 1.62-5.69; P = 0.001) and a non-usual coronary artery anatomy (HR = 2.41, 95% CI 1.45-4.00; P = 0.001). One hundred and one catheter interventions were performed in 54 patients, usually for relief of supravalvular pulmonary stenosis (44/54 patients, 81.5%) or arch obstruction (10/54 patients, 18.5%). Main risk factor for catheter intervention on multivariable analysis was aortic arch repair associated with ASO (HR = 2.95, 95% CI 1.37-6.36; P = 0.006). Significant coronary artery stenosis was relatively uncommon (9/413 patients, 2.2%) but may be underrepresented.
Patients after ASO typically have good long-term clinical outcomes but reoperations and interventions remain necessary in some patients. Neoaortic valve regurgitation with root dilatation is the second most common indication for reoperation after right ventricular outflow tract obstruction and an increasing need for neoaortic valve and root redo surgery in future is to be expected.
本研究旨在通过分析心脏转归指标(住院和晚期死亡率、再次手术和导管介入、严重冠状动脉阻塞),并确定再次手术和导管介入的风险因素,评估我们 43 年来对大动脉转位(TGA)进行动脉调转手术(ASO)的经验。
本回顾性单中心研究纳入了 1977 年至 2020 年间接受 ASO 治疗 TGA 的 490 例患者。通过 Kaplan-Meier 方法估计医院幸存者的再次手术和导管介入数据,并使用长期秩检验进行比较。通过多变量 Cox 回归分析评估再次手术和/或导管介入的风险因素。
43 例(8.8%)患者发生院内死亡,12 例(2.9%)患者发生晚期死亡,43 例患者失访。413 例存活于医院的患者的中位随访时间为 15.6(四分位间距 7.0-22.4)年。83 例患者(117 次再次手术)进行了再次手术。右心室流出道梗阻(50/83 例,60.2%)后,新发主动脉瓣反流伴根部扩张是再次手术的第二大常见指征(15/83 例,18.1%)。多变量分析的任何再次手术的风险因素包括:TGA 形态学亚型[伴有室间隔缺损的 TGA:风险比(HR)=1.99,95%置信区间(CI)1.18-3.36;P=0.010 和 Taussig-Bing:HR=2.17,95%CI 1.02-4.64;P=0.045]、ASO 时合并主动脉弓修复(HR=3.03,95%CI 1.62-5.69;P=0.001)和非典型冠状动脉解剖(HR=2.41,95%CI 1.45-4.00;P=0.001)。54 例患者(54 次导管介入)进行了 101 次导管介入,通常用于缓解瓣上型肺动脉狭窄(44/54 例,81.5%)或弓部梗阻(10/54 例,18.5%)。多变量分析的导管介入的主要风险因素是 ASO 时合并主动脉弓修复(HR=2.95,95%CI 1.37-6.36;P=0.006)。严重冠状动脉狭窄相对少见(413 例患者中有 9 例,2.2%),但可能被低估。
ASO 后患者通常具有良好的长期临床转归,但一些患者仍需要再次手术和介入治疗。新发主动脉瓣反流伴根部扩张是继右心室流出道梗阻之后的第二大再次手术指征,未来预计需要更多的主动脉瓣和根部再次手术。