Program On Regulation, Therapeutics, And Law, Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital, Boston, Massachusetts.
Harvard Medical School, Boston, Massachusetts.
JAMA Netw Open. 2021 May 3;4(5):e218816. doi: 10.1001/jamanetworkopen.2021.8816.
List prices set by manufacturers for brand-name prescription drugs in the US have been increasing faster than inflation, although confidential manufacturer rebates offset some of these increases. Most commercially insured patients pay at least some out-of-pocket costs for prescription drugs, and higher patient spending is associated with lower adherence and worse health outcomes.
To examine whether price changes for brand-name drugs are correlated with changes in patient out-of-pocket spending and whether this association varies by insurance benefit design.
DESIGN, SETTING, AND PARTICIPANTS: A cohort study of 79 brand-name drugs with available pricing data from January 2015 to December 2017 was conducted, with data obtained from a national commercial insurance claims database.
Change in the list prices set by manufacturers and estimated net prices after rebates among non-Medicaid payers.
Change in median out-of-pocket spending among all patients and stratified by insurance pharmacy benefit design, including high-deductible insurance plans and plans with any amount of deductibles or coinsurance.
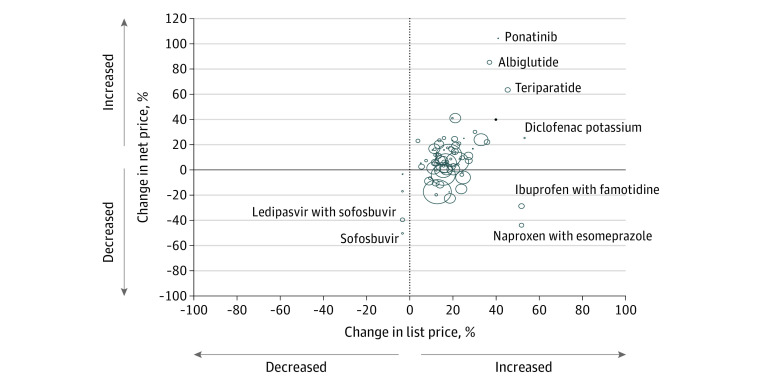
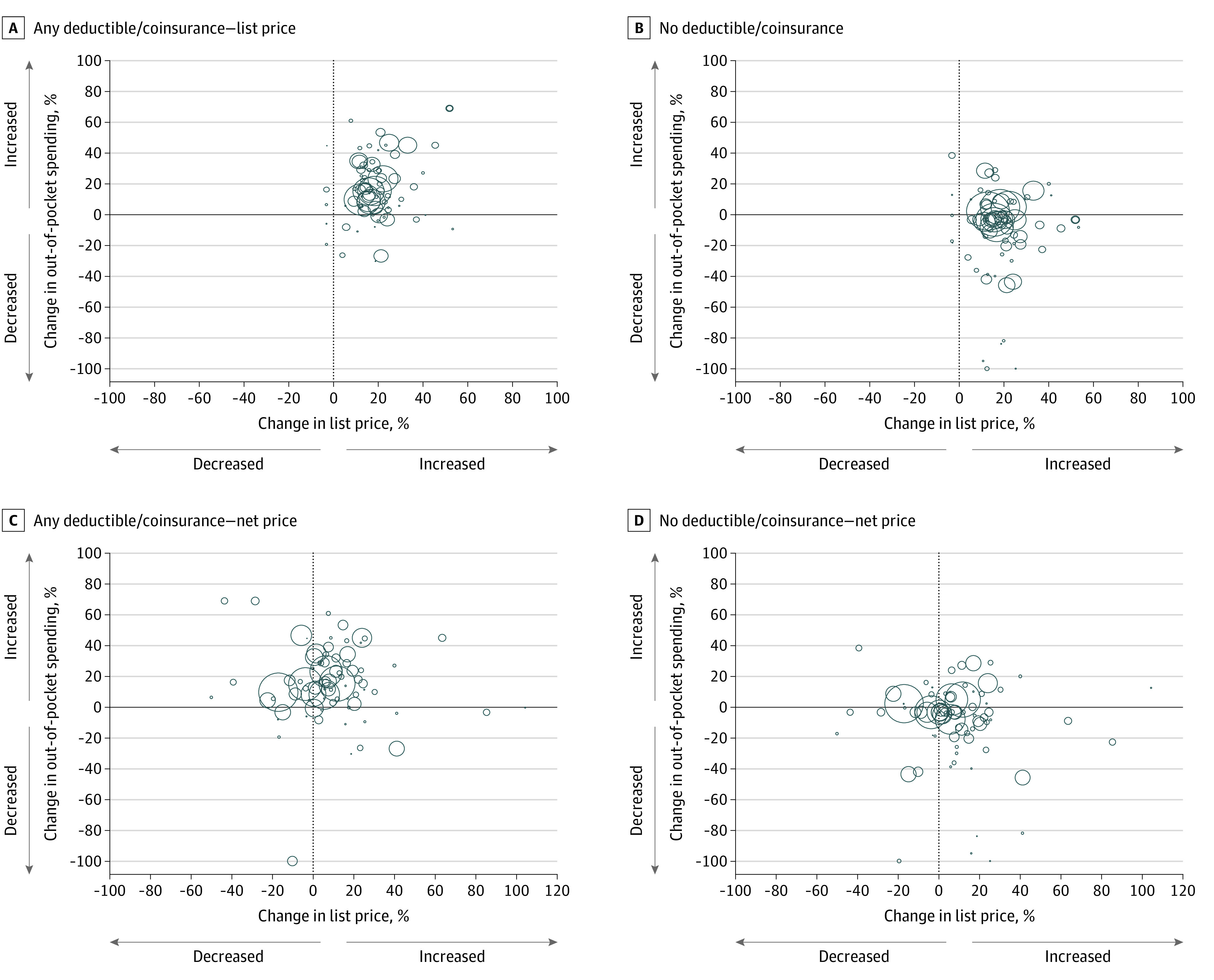
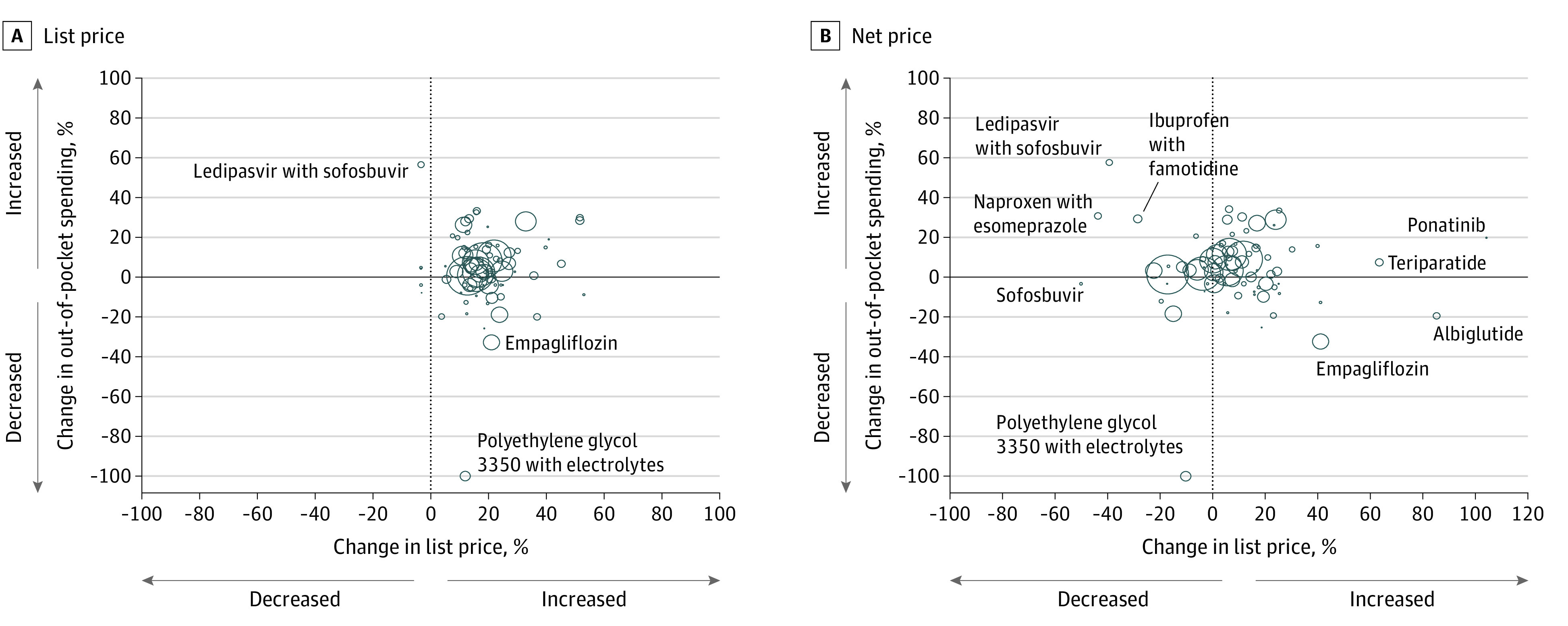
Among 79 drugs, median increases were 16.7% (interquartile range [IQR], 13.6%-21.1%) for list prices, 5.4% (IQR, -3.9% to 11.7%) for net prices, and 3.5% (IQR, 1.4%-9.1%) for out-of-pocket spending from 2015 to 2017. Changes in list prices were correlated with changes in net prices (r = 0.34; P = .002). Overall, changes in out-of-pocket spending were not correlated with changes in list prices (r = 0.14; P = .22) or net prices (r = 0.04; P = .71). Among 53.7% of patients who paid any drug deductible or coinsurance, median out-of-pocket spending increased by 15.0%, and changes were moderately correlated with changes in list prices (r = 0.38; P = .001) but not net prices (r = 0.06; P = .62).
Some commercially insured patients who pay only prescription drug copayments appear to be insulated from increases in drug prices. However, more than half of patients pay deductibles or coinsurance and may experience substantial increases in out-of-pocket spending when drug prices increase. Among these patients, there was no evidence that manufacturer rebates to insurers are associated with patients' out-of-pocket spending. Policies to rein in unregulated annual increases in list prices for brand-name drugs may have important consequences for patient out-of-pocket spending.
美国品牌处方药制造商设定的目录价格一直在上涨,超过了通胀水平,尽管制造商的秘密回扣抵消了部分涨幅。大多数有商业保险的患者在购买处方药时至少要支付一些自付费用,而较高的患者自付费用与较低的依从性和较差的健康结果有关。
研究品牌药品价格变化是否与患者自付费用的变化相关,以及这种关联是否因保险福利设计而异。
设计、地点和参与者:这是一项队列研究,纳入了 79 种有定价数据的品牌药品,研究数据来自全国商业保险理赔数据库,研究时间为 2015 年 1 月至 2017 年 12 月。
非医疗补助支付者制造商设定的目录价格和回扣后估计的净价格变化。
所有患者(按保险药房福利设计分层,包括高免赔额保险计划和有任何免赔额或共付额的计划)的中位数自付支出变化。
在 79 种药品中,目录价格中位数增长 16.7%(四分位距[IQR],13.6%-21.1%),净价格中位数增长 5.4%(IQR,-3.9%-11.7%),自付支出中位数增长 3.5%(IQR,1.4%-9.1%),2015 年至 2017 年。目录价格的变化与净价格的变化相关(r=0.34;P=0.002)。总体而言,自付支出的变化与目录价格(r=0.14;P=0.22)或净价格(r=0.04;P=0.71)的变化无关。在 53.7%的支付任何药品免赔额或共同保险的患者中,自付支出中位数增加了 15.0%,变化与目录价格的变化中度相关(r=0.38;P=0.001),但与净价格的变化无关(r=0.06;P=0.62)。
一些只支付处方药共付额的商业保险患者似乎免受药品价格上涨的影响。然而,超过一半的患者支付免赔额或共同保险,当药品价格上涨时,他们的自付支出可能会大幅增加。在这些患者中,没有证据表明制造商向保险公司的回扣与患者的自付支出有关。对品牌药品目录价格不受监管的年度上涨进行管控的政策可能对患者自付支出产生重要影响。