Pathology, Institute of Medical Genetics and Pathology, University Hospital Basel, University of Basel, Basel, Switzerland.
Institute of Medical Genetics and Pathology, Schönbeinstraße 40, 4031, Basel, Switzerland.
Pathologe. 2021 Nov;42(Suppl 1):89-97. doi: 10.1007/s00292-021-00945-6. Epub 2021 May 5.
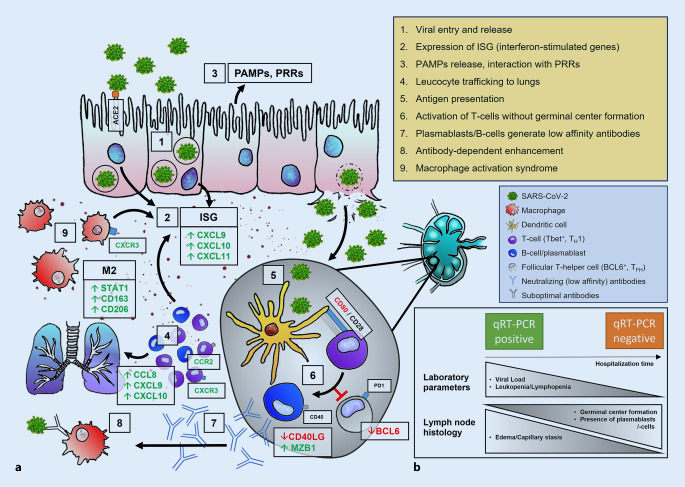
A dysregulated immune response is considered one of the major factors leading to severe COVID-19. Previously described mechanisms include the development of a cytokine storm, missing immunoglobulin class switch, antibody-mediated enhancement, and aberrant antigen presentation.
To understand the heterogeneity of immune response in COVID-19, a thorough investigation of histomorphological patterns in regional lymph nodes was performed.
Lymph nodes from the cervical, mediastinal, and hilar regions were extracted from autopsies of patients with lethal COVID-19 (n = 20). Histomorphological characteristics, SARS-CoV‑2 qRT-PCR, and gene expression profiling on common genes involved in immunologic response were analyzed.
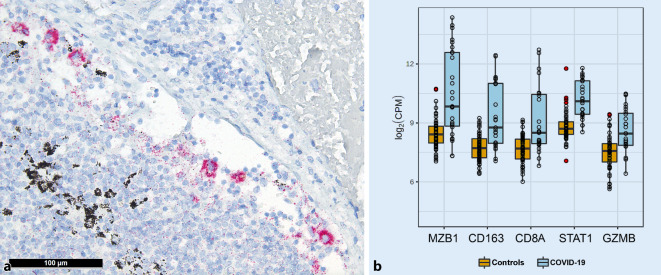
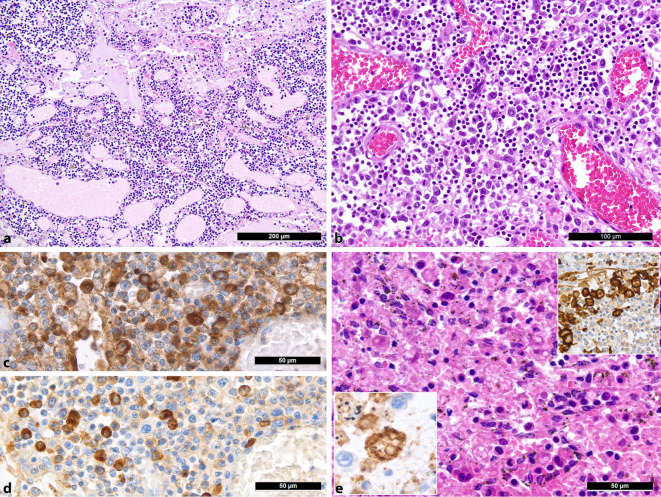
Lymph nodes displayed moderate to severe capillary stasis and edema, an increased presence of extrafollicular plasmablasts, mild to moderate plasmacytosis, a dominant population of CD8 T‑cells, and CD11c/CD68 histiocytosis with hemophagocytic activity. Out of 20 cases, 18 presented with hypoplastic or missing germinal centers with a decrease of follicular dendritic cells and follicular T‑helper cells. A positive viral load was detected by qRT-PCR in 14 of 20 cases, yet immunohistochemistry for SARS-CoV-2 N-antigen revealed positivity in sinus histiocytes of only one case. Gene expression analysis revealed an increased expression of STAT1, CD163, granzyme B, CD8A, MZB1, and PAK1, as well as CXCL9.
Taken together, our findings imply a dysregulated immune response in lethal COVID-19. The absence/hypoplasia of germinal centers and increased presence of plasmablasts implies a transient B‑cell response, implying an impaired development of long-term immunity against SARS-CoV‑2 in such occasions.
免疫反应失调被认为是导致严重 COVID-19 的主要因素之一。先前描述的机制包括细胞因子风暴的发展、免疫球蛋白类别转换缺失、抗体介导的增强以及异常抗原呈递。
为了了解 COVID-19 中免疫反应的异质性,对区域性淋巴结的组织形态模式进行了彻底调查。
从致死性 COVID-19 患者(n=20)的尸检中提取颈、纵隔和肺门区域的淋巴结。分析组织形态学特征、SARS-CoV-2 qRT-PCR 和常见免疫反应相关基因的基因表达谱。
淋巴结显示中等至重度毛细血管淤滞和水肿,滤泡外浆母细胞增多,轻度至中度浆细胞增多,CD8 T 细胞占主导地位,CD11c/CD68 组织细胞伴有噬血细胞活性。在 20 例中,有 18 例表现为生发中心发育不良或缺失,滤泡树突状细胞和滤泡辅助性 T 细胞减少。qRT-PCR 检测到 14 例中有阳性病毒载量,但 SARS-CoV-2 N 抗原的免疫组化仅在 1 例中显示阳性。基因表达分析显示 STAT1、CD163、颗粒酶 B、CD8A、MZB1 和 PAK1 以及 CXCL9 的表达增加。
综上所述,我们的发现表明致命性 COVID-19 中存在免疫反应失调。生发中心的缺失/发育不良和浆母细胞的增多暗示着短暂的 B 细胞反应,这意味着在这种情况下对 SARS-CoV-2 产生长期免疫的能力受损。