Pathology, Institute of Medical Genetics and Pathology, University Hospital Basel, University of Basel, Basel, Switzerland.
Department of Biomedicine, University of Basel, Basel, Switzerland.
Front Immunol. 2021 Dec 13;12:763098. doi: 10.3389/fimmu.2021.763098. eCollection 2021.
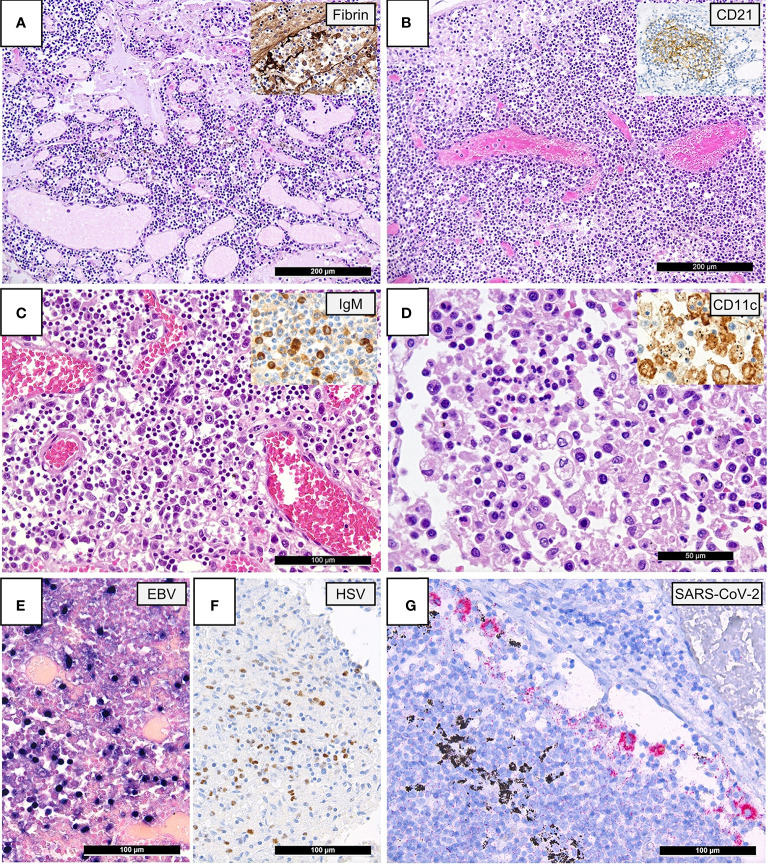
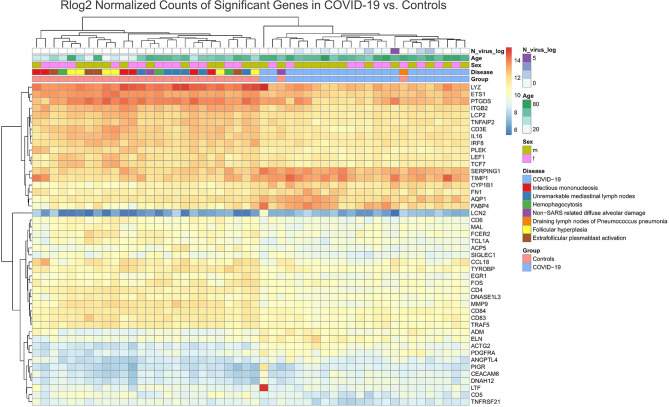
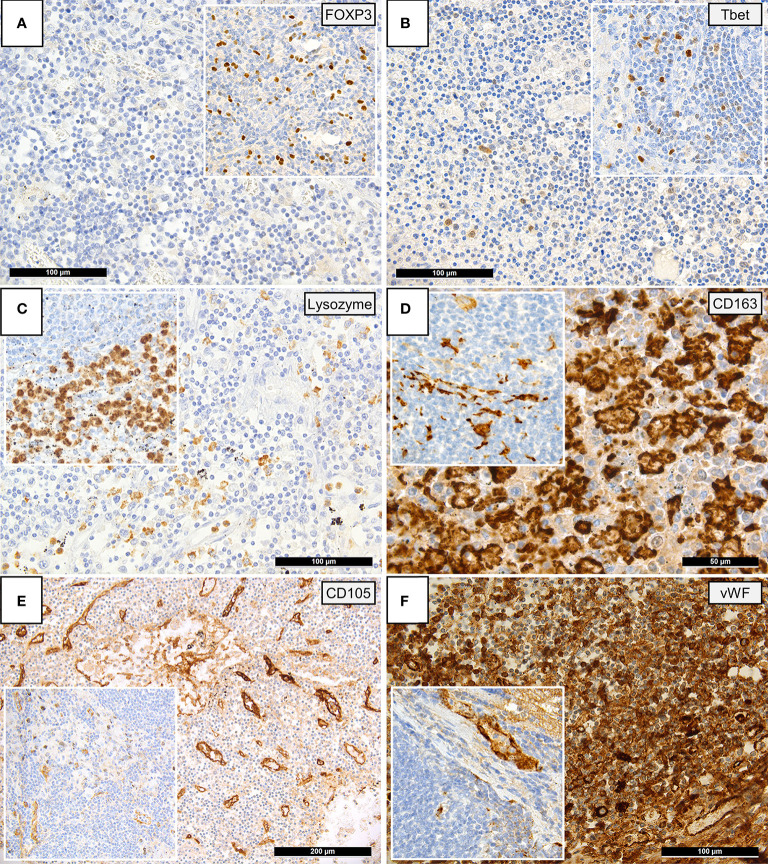
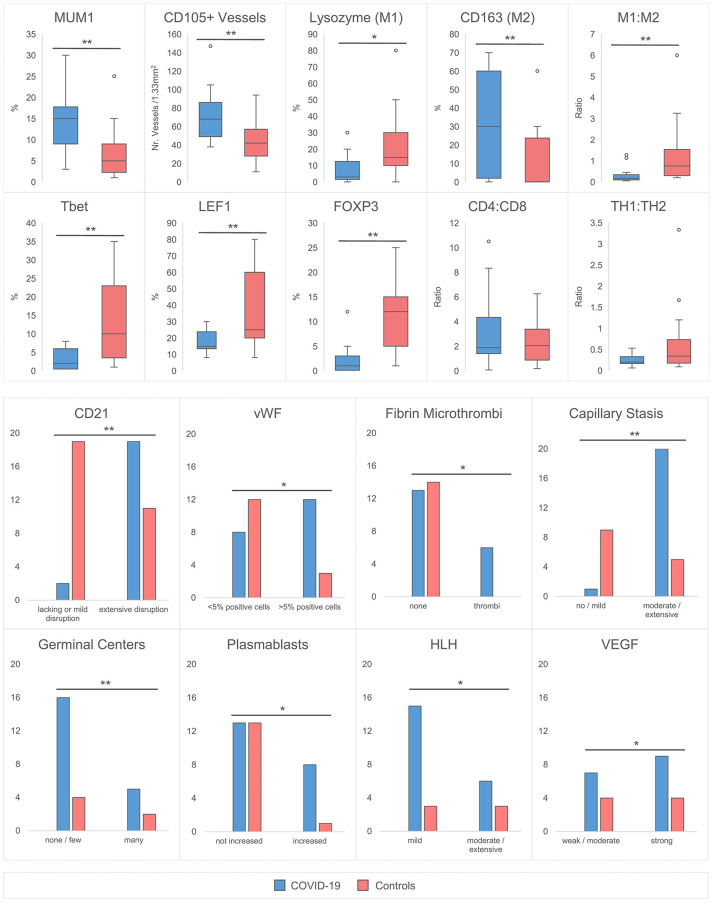
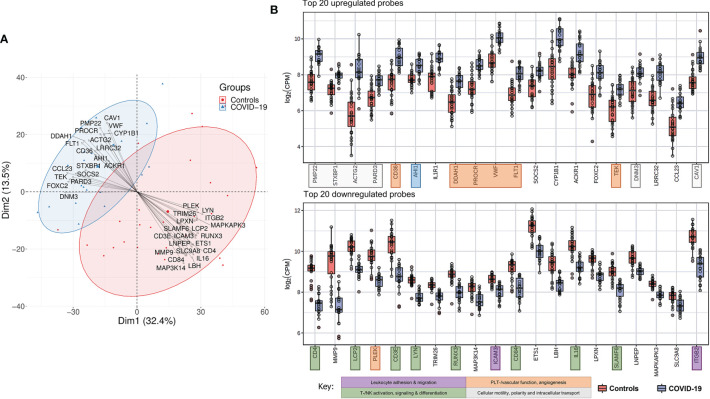
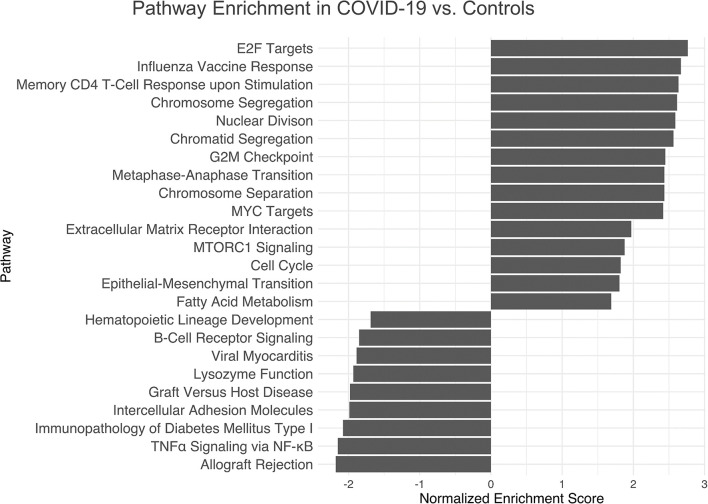
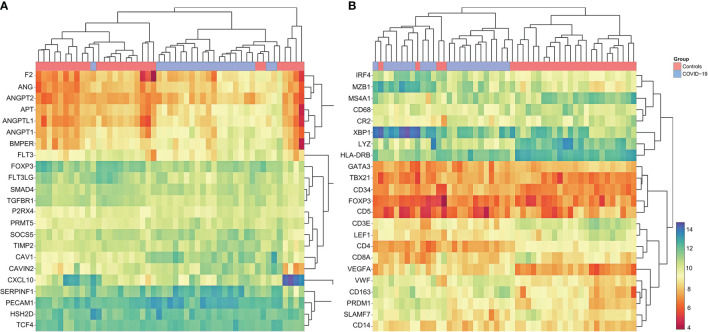
Although initial immunophenotypical studies on peripheral blood and bronchoalveolar lavage samples have provided a glimpse into the immunopathology of COVID-19, analyses of pulmonary draining lymph nodes are currently scarce. 22 lethal COVID-19 cases and 28 controls were enrolled in this study. Pulmonary draining lymph nodes (mediastinal, tracheal, peribronchial) were collected at autopsy. Control lymph nodes were selected from a range of histomorphological sequelae [unremarkable histology, infectious mononucleosis, follicular hyperplasia, non-SARS related HLH, extrafollicular plasmablast activation, non-SARS related diffuse alveolar damage (DAD), pneumonia]. Samples were mounted on a tissue microarray and underwent immunohistochemical staining for a selection of immunological markers and hybridization for Epstein Barr Virus (EBV) and SARS-CoV-2. Gene expression profiling was performed using the HTG EdgeSeq Immune Response Panel. Characteristic patterns of a dysregulated immune response were detected in COVID-19: 1. An accumulation of extrafollicular plasmablasts with a relative paucity or depletion of germinal centers. 2. Evidence of T-cell dysregulation demonstrated by immunohistochemical paucity of FOXP3+, Tbet+ and LEF1+ positive T-cells and a downregulation of key genes responsible for T-cell crosstalk, maturation and migration as well as a reactivation of herpes viruses in 6 COVID-19 lymph nodes (EBV, HSV). 3. Macrophage activation by a M2-polarized, CD163+ phenotype and increased incidence of hemophagocytic activity. 4. Microvascular dysfunction, evidenced by an upregulation of hemostatic (CD36, PROCR, VWF) and proangiogenic (FLT1, TEK) genes and an increase of fibrin microthrombi and CD105+ microvessels. Taken together, these findings imply widespread dysregulation of both innate and adoptive pathways with concordant microvascular dysfunction in severe COVID-19.
尽管对外周血和支气管肺泡灌洗液样本的初步免疫表型研究提供了对 COVID-19 免疫病理学的初步了解,但对肺引流淋巴结的分析目前还很少。本研究纳入了 22 例致命性 COVID-19 病例和 28 例对照。尸检时收集肺引流淋巴结(纵隔、气管、支气管旁)。对照淋巴结选自一系列组织形态学后遗症[无明显组织学改变、传染性单核细胞增多症、滤泡增生、非 SARS 相关 HLH、滤泡外浆母细胞激活、非 SARS 相关弥漫性肺泡损伤(DAD)、肺炎]。样本被安装在组织微阵列上,并进行了一系列免疫标志物的免疫组织化学染色和 EBV 和 SARS-CoV-2 的杂交。使用 HTG EdgeSeq 免疫反应面板进行基因表达谱分析。在 COVID-19 中检测到失调免疫反应的特征模式:1. 滤泡外浆母细胞的积累,而生发中心相对稀少或耗竭。2. 通过 FOXP3+、Tbet+和 LEF1+阳性 T 细胞的免疫组织化学稀少和负责 T 细胞串扰、成熟和迁移的关键基因的下调以及 6 例 COVID-19 淋巴结中疱疹病毒的重新激活(EBV、HSV),证明 T 细胞失调。3. M2 极化、CD163+表型的巨噬细胞激活和噬血细胞活性增加。4. 微血管功能障碍,表现为止血(CD36、PROCR、VWF)和促血管生成(FLT1、TEK)基因的上调以及纤维蛋白微血栓和 CD105+微脉管的增加。总之,这些发现表明严重 COVID-19 中先天和适应性途径广泛失调,伴有一致的微血管功能障碍。